ABSTRACT
Objective: To estimate the economic burden of posttraumatic stress disorder (PTSD) in the United States civilian and military populations from a societal perspective.
Methods: A prevalence-based and human capital approach was used to estimate the total excess costs of PTSD in 2018 from insurance claims data, academic literature, and governmental publications. Excess direct health care costs (pharmacy, medical), direct non–health care costs (research and training, substance use, psychotherapy, homelessness, disability), and indirect costs (unemployment, productivity loss, caregiving, premature mortality) associated with PTSD were compared between adults with PTSD and adults without PTSD, or the general population if information was not available for adults without PTSD.
Results: The total excess economic burden of PTSD in the US was estimated at $232.2 billion for 2018 ($19,630 per individual with PTSD). Total excess costs were $189.5 billion (81.6%) in the civilian population and $42.7 billion (18.4%) in the military population, corresponding to $18,640 and $25,684 per individual with PTSD in the civilian and military populations, respectively. In the civilian population, the excess burden was driven by direct health care ($66.0 billion) and unemployment ($42.7 billion) costs. In the military population, the excess burden was driven by disability ($17.8 billion) and direct health care ($10.1 billion) costs.
Conclusions: The economic burden of PTSD goes beyond direct health care costs and has been found to rival costs for other costly mental health conditions. Increased awareness of PTSD, development of more effective therapies, and expansion of evidence-based interventions may be warranted to reduce the large clinical and economic burden of PTSD.
J Clin Psychiatry 2022;83(3):21m14116
To cite: Davis LL, Schein J, Cloutier M, et al. The economic burden of posttraumatic stress disorder in the United States from a societal perspective. J Clin Psychiatry. 2022;83(3):21m14116.
To share: https://doi.org/10.4088/JCP.21m14116
© Copyright 2022 Physicians Postgraduate Press, Inc.
aResearch Service, Tuscaloosa Veterans Affairs Medical Center, Tuscaloosa, Alabama
bDepartment of Psychiatry, University of Alabama School of Medicine, Birmingham, Alabama
cOtsuka Pharmaceutical Development & Commercialization, Inc., Princeton, New Jersey
dAnalysis Group, Inc., Montréal, Quebec
eLundbeck LLC, Deerfield, Illinois
*Corresponding author: Lori L. Davis, MD, Research Service, Tuscaloosa Veterans Affairs Medical Center, 3701 Loop Rd East, Tuscaloosa, AL 35404 ([email protected]).
Posttraumatic stress disorder (PTSD) can develop after witnessing or experiencing a traumatic event, such as life-threatening or sexually traumatic events,1 and can cause long-term disability and premature morbidity and mortality.1–3 Symptoms include intrusive thoughts and nightmares related to the trauma, mental and/or physical distress to trauma-related stimuli, avoidant behaviors, negative thoughts and feelings, and hyperarousal symptoms.1 Management of PTSD involves psychological and/or pharmacologic options based on clinical judgment and patient preference.4 Various PTSD treatment guidelines (eg, US Department of Veterans Affairs and Department of Defense, World Health Organization) support trauma-focused psychotherapy as first-line treatment for PTSD, which aims to emotionally process the traumatic memory and integrate new information so that the trauma reminder is no longer seen as a signal of threat.1,5,6 As for pharmacotherapy, barriers to treatment exist, with many individuals remaining untreated7 and only two pharmacologic agents (both antidepressants) approved for the treatment of PTSD by the US Food and Drug Administration (FDA) in the past 20 years.8 In addition, stigmatization of PTSD further contributes to the barriers to treatment.9,10 Particularly if left untreated or only partially responsive,1,11 PTSD is associated with an increased risk of substance use disorder (SUD), disability, unemployment, and premature mortality, all of which contribute to a substantial clinical burden.2,3,12,13
In line with the clinical burden, PTSD is also associated with a substantial economic burden. However, there is limited literature describing the total economic burden of PTSD in the US. Studies mostly focus on the military population and/or are limited to direct health care costs.14–18 While the prevalence of PTSD in the US is higher in the military population than in the civilian population, the military population composes only a small proportion of the overall US population.19 Together with the fact that PTSD is known to be underdiagnosed and undertreated,7,20 existing reports of the economic burden of PTSD are likely not capturing the actual burden of the disease. To address this gap in knowledge and to inform stakeholders, this study provides a contemporary and comprehensive evaluation of the total direct health care, direct non–health care, and indirect costs associated with PTSD in both US civilian and US military (ie, active military and Veteran) populations from a societal perspective.
METHODS
Data Source
IBM MarketScan Commercial, Medicare Supplemental, and Multi-State Medicaid Databases were used to obtain the direct health care costs of PTSD among the civilian population. Direct health care costs of PTSD in the military population and direct non–health care and indirect costs in the civilian and military populations were estimated based on the literature, including data from the US Census and governmental agencies. Each source was chosen in consultation with clinical experts to identify credible and accurate estimates based on a targeted evaluation of the data reported and relevance for this study. Selected estimates from the literature were those that were deemed of highest relevance to the current study in terms of population studied (eg, adult population, civilian or military patients, US-only), robustness/quality of the estimates (eg, methods, sample size), and recency of the study, compared to other available literature. For the prevalence estimates used to calculate economic burden, results from a systematic literature review were used, which was conducted to identify high-quality studies, based on the generalizability of the results to the study’s targeted population, quality of the measurement of PTSD (eg, clinical interviews versus self-reported surveys), and overall quality of the methodology.21
Excess Economic Burden of PTSD
The total excess economic burden of PTSD in the US for 2018 (the latest year for which data were available at the time of study) was evaluated from a societal perspective based on the average cost differences between an adult with PTSD and an adult without PTSD, or from the general population if the information was not available for adults without PTSD. (The term average represents “mean values” throughout this report.) Each cost component was estimated using a prevalence-based approach. Given that multiple data sources were used in the calculation (Table 1), estimated costs were weighted by the distribution of the relevant individual characteristics in the US population in the year 2018. For example, for publications with male and female stratification, results were reweighted based on the prevalence of PTSD by sex. An adjustment for population growth was used to account for costs derived from statistics published before or after 2018. Cost components were calculated to be mutually exclusive.
Direct health care costs. Costs were weighted by the distribution of adults with each type of health plan (commercial, Medicare, and Medicaid) or no health plan coverage (Table 1). For uninsured individuals, costs were derived based on the portion of medical service costs that were covered by federal, state, and/or local institutions, as well as the private sector in 2018 (ie, uncompensated health care cost).22
For individuals in the military population, costs were estimated from the literature and calculated as the amount reimbursed by the primary payer (ie, Veterans Affairs [VA] or Department of Defense [DOD]). In cases when patients were not covered by VA or DOD plans or only sought medical services outside of the military network, excess health care costs were proxied based on the costs from commercial, Medicare, and Medicaid claims.
Direct non–health care costs. Direct non–health care costs were based on the literature and included costs for research and training on PTSD, SUD, psychotherapy services (ie, only psychotherapy services covered by health plans were included under direct health care costs), homelessness, and disability. Substance use disorder was included as a separate cost component since it is associated with additional costs related to crimes, prevention and research, and road traffic accidents that were not already captured elsewhere (eg, direct health care costs, unemployment) and for which reliable sources were available.13,29–31
Indirect costs. Indirect costs of PTSD were estimated based on the literature and governmental publications using a human capital approach, in which costs were derived using paid work compensation rates.57 Components included unemployment, productivity loss at work (ie, presenteeism and absenteeism), caregiving, and premature mortality.
RESULTS
Using one of the most recent US prevalence estimates of PTSD (civilian population: 2.6% and 6.0% for men and women, respectively; military population: 6.7% and 11.7%, respectively)19 and 2018 population estimates from the Census Bureau,55 VA,56 and DOD,58 2,607,131 male and 7,558,833 female adults were estimated to have PTSD in the US civilian population and 1,368,925 male and 293,256 female adults in the US military population. Female adults with PTSD accounted for 66.4% of the overall PTSD population.
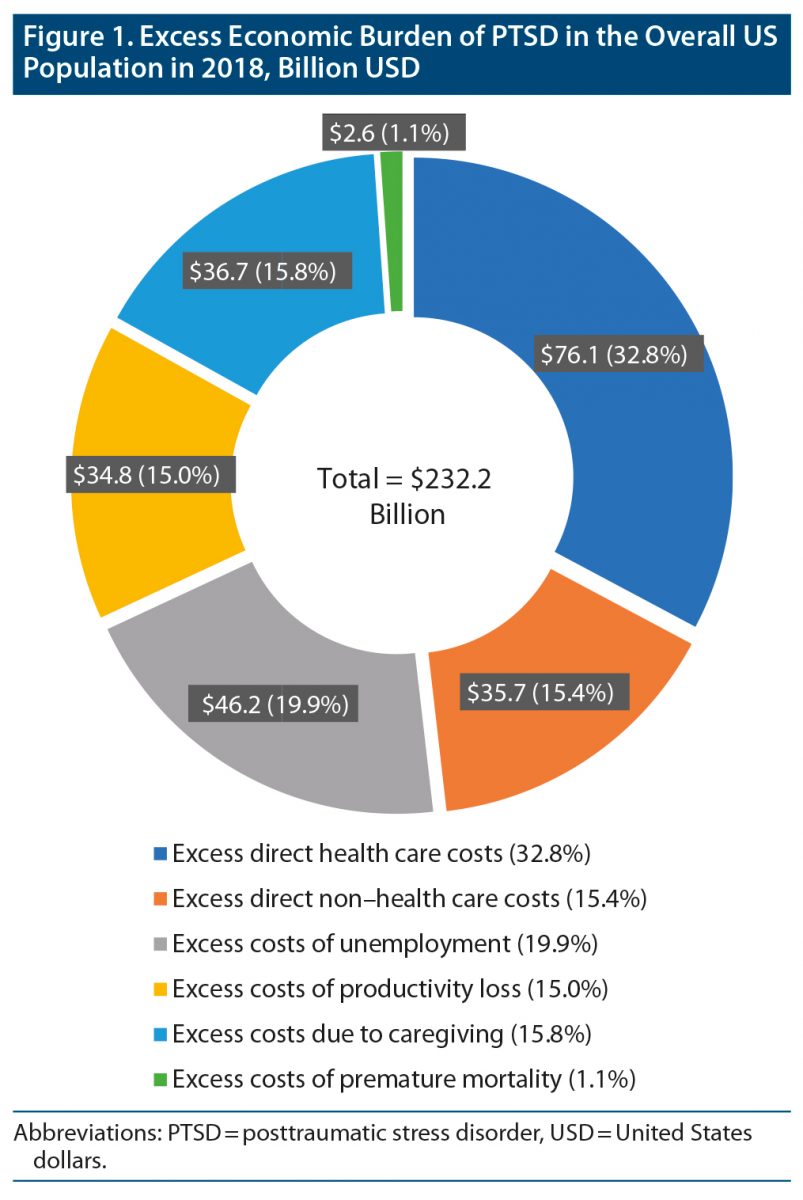
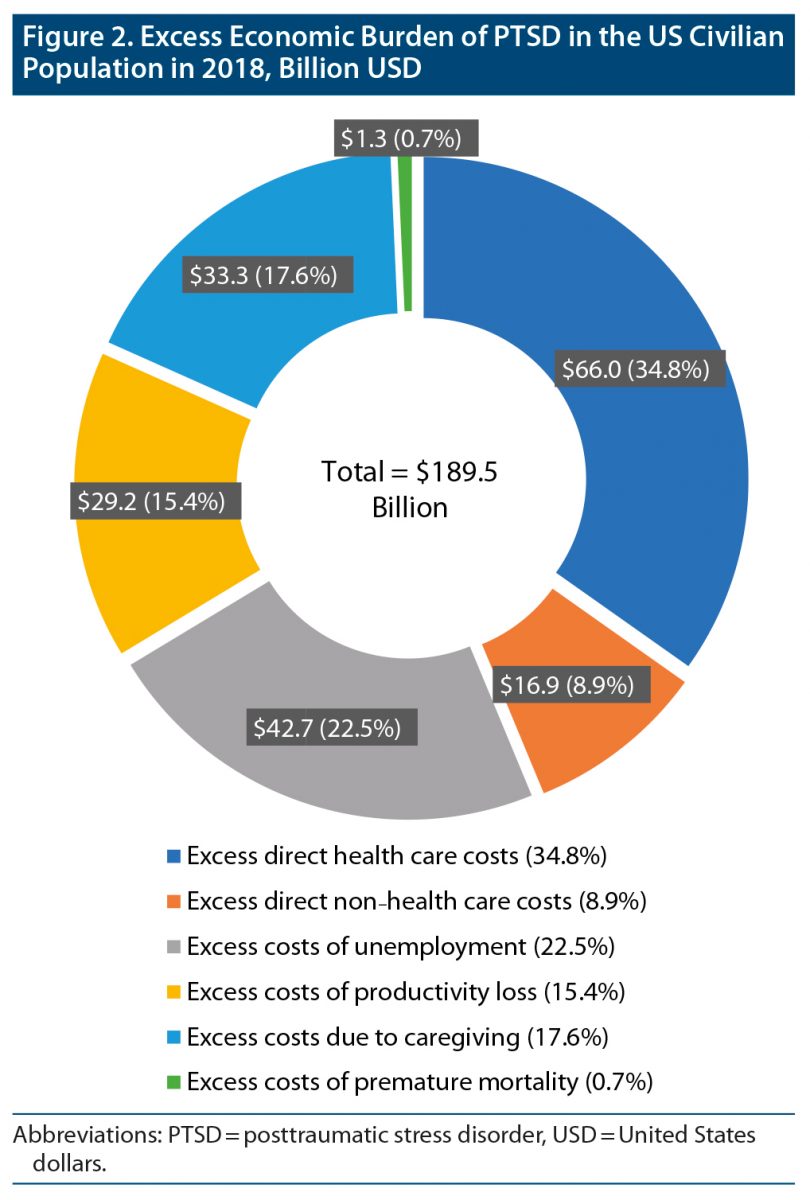
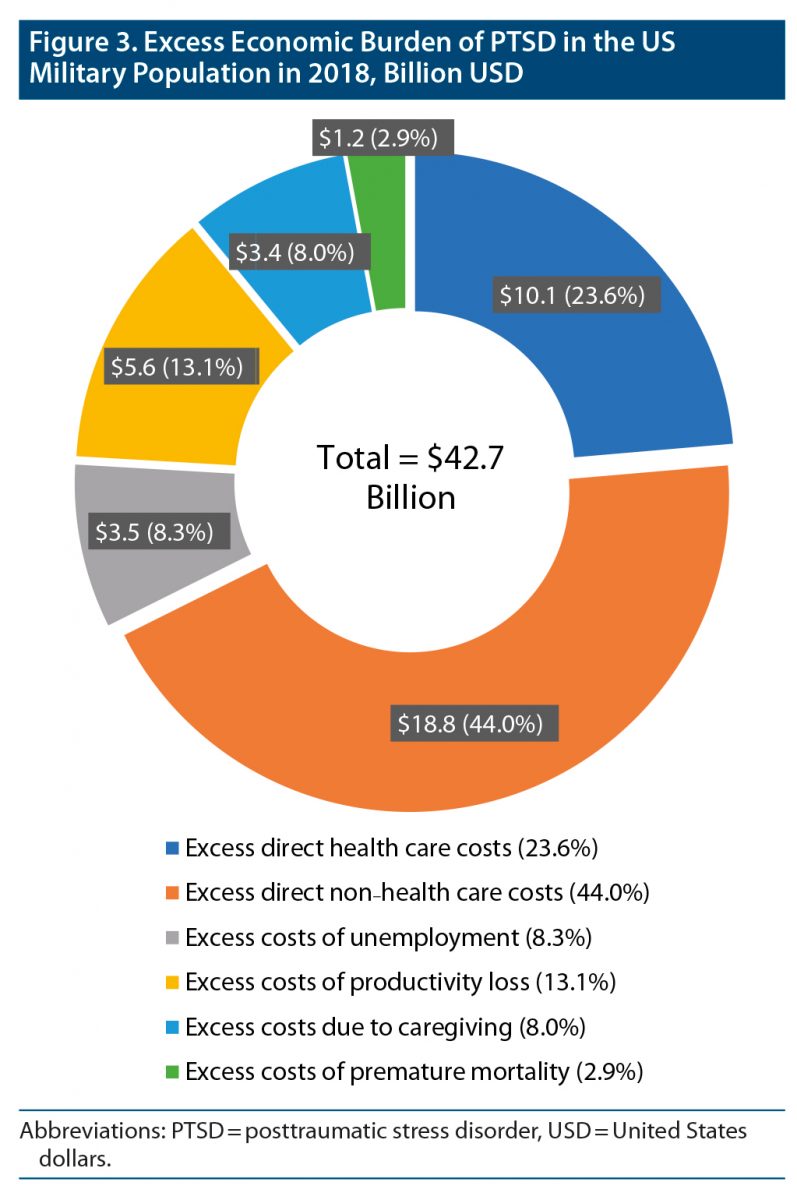
Based on these estimates, the total excess economic burden of PTSD in the US was estimated at $232.2 billion for 2018, corresponding to $19,630 in excess costs annually due to PTSD per individual with PTSD. While a larger proportion of these total excess costs is attributed to the civilian population ($189.5 billion [81.6%]) than the military population ($42.7 billion [18.4%]), the excess costs per individual with PTSD are lower for the civilian population ($18,640) than for the military population ($25,684).
Direct Health Care Costs
Among the civilian and military populations, the average excess direct health care costs ranged from $12,167 to $13,016 per individual with PTSD. Accordingly, across all individuals with PTSD, the total excess direct health care costs of PTSD were estimated at $76.1 billion ($66.0 billion in the US civilian population and $10.1 billion in the US military population; Figure 1, Figure 2, and Figure 3).
Direct Non–Health Care Costs
PTSD-related research and training. The National Institutes of Health and VA/DOD annual PTSD-related research and training costs in the US population in 2018 were estimated at $136.0 million ($96.3 million in the US civilian population and $39.7 million in the US military population).19,27,28
Substance use disorder. Based on the literature, the proportion of civilian adults with PTSD with alcohol use disorder was estimated to be 2.2 times higher than the proportion reported in civilian adults without PTSD; this proportion was 2.4 times higher for drug use disorder.19,30 In the military population, the excess SUD due to PTSD was even more pronounced, with the proportions being 5.8 times and 7.3 times higher for alcohol use and drug use disorders, respectively.13,19 As a result, the excess costs of SUD due to PTSD were $2.3 billion overall ($1.6 billion in the US civilian population and $722.4 million in the US military population).
Psychotherapy services not covered under health plans. The excess rate of psychotherapy utilization due to PTSD was estimated to be 11.6% among uninsured adults in the civilian population, comprising a total of approximately 124,000 additional uninsured individuals seeking psychotherapy services due to PTSD.19,32,33,59 Assuming an average of 10 psychotherapy visits per year for an uninsured individual who seeks psychotherapy services,34 and at an average cost of $133 per 1-hour psychotherapy visit,32 this translates to an estimated $156.2 million in excess costs of psychotherapy due to PTSD among uninsured civilian individuals.
Homelessness. Based on data from 2018, there were approximately 35,000 and 11,000 excess sheltered homeless adults per night in the civilian and military populations, respectively, due to PTSD.35,36,38 Accordingly, the excess costs of homelessness due to PTSD were $869.1 million overall ($660.0 million in the US civilian population and $209.1 million in the US military population).
Disability. Among 1.2 million adults receiving disability benefits for PTSD in the US, 85.9% were from the civilian population and 14.1% from the military population.39 Additionally, an estimated 1.0 million Veterans received VA PTSD-related disability benefits in the US military population.41 Thus, the excess costs of disability benefits due to PTSD were estimated at $32.3 billion overall ($14.5 billion in the US civilian population and $17.8 billion in the US military population). Of note, disability was the single largest contributor of the excess economic burden in the US military population.
Indirect Costs
Unemployment. An additional 10.5% of male adults and 15.8% of female adults were unemployed due to PTSD in the US civilian population compared to the general population without PTSD.12,19,54 In the military population, a smaller excess of 7.0% of male adults and 8.7% of female adults were unemployed due to PTSD.3,19,43 This translates to estimated excess costs of unemployment due to PTSD of $46.2 billion overall ($42.7 billion in the US civilian population and $3.5 billion in the US military population; Figure 1, Figure 2, and Figure 3).44,45
Productivity loss at work. In the general US population, 9.7 and 33.1 excess days per year were lost due to PTSD-related absenteeism and presenteeism, respectively, among adults with PTSD.19,46 Based on these numbers, the excess costs of productivity loss at work due to PTSD were estimated at $34.8 billion overall ($29.2 billion in the US civilian population and $5.6 billion in the US military population; Figure 1, Figure 2, and Figure 3).44,45
Caregiving. In the civilian population, caregivers spent an additional 3.4 hours per week devoted to PTSD-related care.19,48,49 In the military population, an additional 2.1 hours per week were devoted to PTSD-related care.19,48,51,52 As a result, the excess costs of caregiving due to PTSD were estimated at $36.7 billion overall ($33.3 billion in the US civilian population and $3.4 billion in the US military population; Figure 1, Figure 2, and Figure 3).47,50,52
Premature mortality. The annual all-cause mortality rate for the civilian population with PTSD was estimated to be 20% higher than that of the overall US population.2,44,60 In the military population with PTSD, the annual all-cause mortality rate was estimated to be 80% higher than that of the military population without PTSD.2,43,45 This resulted in estimated excess costs of all-cause premature mortality due to PTSD of $2.6 billion overall ($1.3 billion in the US civilian population and $1.2 billion in the US military population; Figure 1, Figure 2, and Figure 3).
DISCUSSION
The $232 billion annual economic burden of PTSD in the US demonstrated in this study is staggering and fuels the urgency for public and private stakeholders to work together to discover new and better treatments, reduce stigma, improve access to existing treatments, and expand evidence-based recovery and rehabilitation programs. The majority of the economic burden was attributed to the civilian population, which incurred $189.5 billion, or 82% of the total costs associated with PTSD.
The economic burden of any illness is driven by many factors, including prevalence, severity, chronicity, access to treatment, and the trajectory of recovery. Much of the research and legislative response on PTSD has focused on combat-exposed populations due to the high prevalence of the condition among the military population.8,61,62 However, the military population composed a small proportion of the overall US population with PTSD (14%), leaving 86% of the PTSD population within civilian groups. With the increasing occurrence of natural and societal traumatic events around the world, including COVID-19,63 civil unrest,64 and climate change,65 there is mounting concern of an increase in PTSD and burden in the civilian population. As such, the current cost estimate is likely an underestimation given these recent global traumas, the effects of which would not have been captured and are likely to result in increasing negative repercussions. Therefore, further research on PTSD among the civilian population is instrumental to address this rapidly accumulating societal burden.
Women represented 66% and 74% of the overall and civilian population with PTSD, respectively, thereby contributing disproportionally to the economic burden. Haller and Chassin66 found that trauma-exposed female individuals exhibit higher levels of PTSD symptoms than trauma-exposed male individuals. Furthermore, traumas such as sexual assault and domestic violence tend to affect more women than men67,68 and represent important areas for prevention and intervention. Although recent public denunciation movements related to sexual assault and domestic violence have brought more awareness to these crimes and their perpetrators, insufficient attention has been given to the impact and lasting effects of PTSD on the survivors of sexual trauma.
The economic burden of PTSD is particularly important to consider in the context of other physical and mental health conditions. The present study found that PTSD incurred higher costs per individual than coronary heart disease and non-serious psychiatric mental illnesses, including anxiety and depressive disorders (Figure 4).69–73 In addition, the excess costs per individual with PTSD for several cost components were lower than those of schizophrenia (eg, direct health care costs, homelessness, unemployment) and higher than those of ADHD (eg, substance abuse, disability). Due to the high prevalence of PTSD relative to other conditions,19 the per individual costs translated to higher total excess costs compared to bipolar disorder or schizophrenia, which have lower prevalence rates (Figure 4).70,71
Notably, major depressive disorder is considered one of the most burdensome mental health conditions affecting working-aged individuals on a global scale, with absenteeism/productivity loss at work being the largest contributor to total costs.75,76 Together with the similar age and sex distribution as PTSD,77,78 this finding suggests that more intentional public health strategies need to be implemented for PTSD, as was done for major depressive disorder, to reduce the stigma, improve treatments, and increase access to care.
The substantial excess burden of PTSD highlights the urgent and unmet need in the treatment and rehabilitation of these individuals. Experts agree that there is a long-standing crisis in pharmacologic drug development for the treatment of PTSD,79 as no medication has been FDA-approved for PTSD since the only two marketed agents were approved 20 years ago.8 Additionally, there is a scarcity of evidence on the impact of available pharmacologic and psychological treatments and the interplay between the two on patient-centered outcomes, such as quality of life, well-being, interpersonal relationships, and occupational functioning.4 A burden that is often ignored in economic calculations is the cost for psychotherapy not covered under health plans, which represents a significant out-of-pocket excess for someone with PTSD, as demonstrated in the current study.
Currently, PTSD is underdiagnosed and even when recognized will often go untreated.7,20 Patients may be reluctant to seek or accept treatment, as many individuals may not associate their symptoms with a mental illness,9 or they may feel a sense of shame and fear of being negatively judged or discriminated against by others.9,10 Additionally, although psychotherapy has demonstrated cost-effectiveness in the treatment of adult civilian patients with PTSD,80,81 individuals may wish to avoid recalling the trauma, and while avoidance is a core symptom of PTSD, recalling the trauma is also typically a necessary component involved in psychotherapy interventions.9,10 As such, there is a need for improved mental health literacy and awareness to reduce the stigmatization and negative perceptions of trauma and PTSD, in turn facilitating the search for and use of appropriate mental health services, which may help to alleviate the burden of PTSD. Additionally, primary care providers and community providers may benefit from increased cognizance of PTSD screening tools, which require little clinical training and could be made available online, as well as treatments for their patients, especially with the recent development of new psychotherapies like written exposure therapy.82
Studies have shown that PTSD symptoms may predict subsequent drug and alcohol problems as a way to self-medicate and manage symptoms of PTSD, thus increasing the risk for SUD.66,83,84 PTSD and SUD are highly correlated, with 46% of adults with PTSD also suffering from SUD.85 PTSD treatment may not only improve PTSD symptoms, but also reduce the burden of comorbid SUD, which, in itself, is a debilitating condition with severe clinical and economic consequences.86,87 Furthermore, given the link between mental illness, substance use, the corresponding high health care costs, and socioeconomic factors like unemployment, homelessness, and disability,35,38,87–90 appropriate PTSD treatment has the potential to reduce the overlapping excess direct health care, non–health care, and indirect burden observed in the current study.
The cost impact of premature mortality associated with PTSD appears proportionally low in our calculation. However, death, particularly by suicide, is devastating to the families left behind, and the associated cost for this loss is not easily calculable. The literature on the risk predictors, interventions, and associations between PTSD and suicide has grown exponentially over the past decade2,91–93; however, research in military populations is dominant,94 and more work is needed in the civilian population to understand and reduce the risk and rates of suicide in people recovering from PTSD.
Finally, the costs of unemployment and productivity loss make up 35% of the total excess economic burden of PTSD in our study. If disability costs are factored in, the proportion approaches half of the total excess economic burden of PTSD. This cost is highly modifiable, considering evidence-based rehabilitation approaches, such as Individual Placement and Support (IPS), that are successful in returning Veterans with disabling PTSD back to steady employment with better incomes, which ultimately yields higher tax revenues for society and improved individual quality of life.95–97 Similar resources and efforts to provide IPS for the civilian population, and particularly women, may universally help improve employment and occupational outcomes and reduce disability for a large sector of the population. As people with PTSD return to work and achieve more independence, the need for a caregiver is also reduced, which has additional cost savings. Furthermore, disability is of particular note in the military population, as it was the single largest contributor of the excess economic burden in this population in the current study, driving the high direct non–health care costs observed. Improvements in the identification and treatment of PTSD may lead to significant government savings, and more importantly, more productive lives for Veterans.
Limitations
For the analysis of excess direct health care costs from claims data, individuals were identified based on a documented diagnosis of PTSD, which may not be representative of those who are undiagnosed. For all cost components, the method used to identify patients with PTSD may result in the misclassification of patients as PTSD case patients or non-case patients. For example, reliance on ICD codes to identify patients with PTSD may result in misclassification of some patients with PTSD as non-case patients if they do not receive a diagnostic code for PTSD and some patients without PTSD as case patients. However, for direct health care costs, patients were required to have two documented diagnoses of PTSD to avoid capturing ICD codes that were used as rule-out diagnoses and thus help to reduce the extent of misclassification in this study. The estimation of excess direct non–health care costs and indirect costs was limited by data availability in the literature. Additionally, since cost components were calculated to be mutually exclusive, the true burden of each component may have been underestimated if it was partially covered by another component. For example, the cost attributed to SUD included only the costs of crimes, prevention and research, and motor vehicle crashes related to substance use, but did not consider incremental medical costs or unemployment that may have resulted from SUD. Moreover, the PTSD prevalence estimates used in this study were based on a narrow definition of PTSD, which may have contributed to underestimation of the total economic burden. Conversely, some cost components may also have been overestimated. For example, residual costs associated with the trauma itself, rather than with PTSD, could have been captured (eg, work loss or medical costs to treat an injury from the trauma). Lastly, since there was no single data source for costs related to PTSD, multiple data sources using different methods, study designs, and populations were combined to estimate the total economic burden of PTSD.
CONCLUSION
The economic burden of PTSD goes beyond direct health care costs and has been found to be quite substantial, exceeding costs for other mental health conditions such as anxiety and depressive disorders. The civilian population, specifically women, has been underrecognized in the literature as a disproportional group suffering from PTSD. Increased awareness of PTSD, development of more effective therapies, and expansion of evidence-based interventions are warranted to reduce the large disease and economic burden of PTSD.
Submitted: May 31, 2021; accepted January 31, 2022.
Published online: April 25, 2022.
Author contributions: Dr Davis, Mr Gagnon-Sanschagrin, Mr Cloutier, Ms Maitland, Ms Guerin, Mr Lefebvre, Dr Schein, Dr Houle, and Ms Urganus contributed to the design of the study and interpretation of the data. Mr Gagnon-Sanschagrin, Mr Cloutier, Ms Maitland, Ms Guerin, and Mr Lefebvre contributed to the data collection and data analysis. All authors critically revised the draft manuscript and approved the final content.
Relevant financial relationships: Over the past 3 years, Dr Davis has received consulting fees from Boehringer Ingelheim, Signant Health, Otsuka, Lundbeck, and Janssen Pharmaceuticals and research funding and/or materials from Tonix Pharmaceuticals, Aptinyx, Social Finance, and Pharmacotherapies for Alcohol and Substance Abuse Consortium funded by US Department of Defense, Veterans Health Administration, and Substance Abuse and Mental Health Services Administration. Mr Gagnon-Sanschagrin, Mr Cloutier, Ms Maitland, Ms Guerin, and Mr Lefebvre are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Otsuka Pharmaceutical Development & Commercialization, Inc., which funded the development and conduct of this study and manuscript. Dr Schein is an employee of Otsuka Pharmaceutical Development & Commercialization, Inc. Dr Houle and Ms Urganus are employees of Lundbeck LLC.
Funding/support: This study was funded by Otsuka Pharmaceutical Development & Commercialization, Inc. and Lundbeck LLC. This material is the result of work supported, in part, with resources at the Tuscaloosa VA Medical Center, Tuscaloosa, Alabama.
Role of the sponsor: Otsuka Pharmaceutical Development & Commercialization, Inc. and Lundbeck LLC contributed to and approved the study design, participated in the interpretation of data, and reviewed and approved the manuscript; all authors contributed to the development of the manuscript and maintained control over the final content.
Disclaimer: Contents do not represent the views of the US Department of Veterans Affairs or the United States Government.
Previous presentation: Part of the material in this manuscript was presented at the Academy of Managed Care Pharmacy (AMCP) 2021 Virtual Meeting from April 12–16 as a poster presentation.
Acknowledgments: Medical writing assistance was provided by Christine Tam, MSc, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Otsuka Pharmaceutical Development & Commercialization, Inc.
Additional information: Ethics statement. For the calculation of direct health care costs among the civilian population, data were de-identified and comply with the patient requirements of the Health Insurance Portability and Accountability Act (HIPAA) of 1996; therefore, no reviews by an institutional review board were required. For all other analyses, only aggregate population-based data were used; patient-level data were not used in this study. Data availability. The data sets generated from the IBM MarketScan Commercial, Medicare Supplemental, and Multi-State Medicaid Databases and analyzed during the current study were used pursuant to a data use agreement and are not publicly available. The data are available through requests made directly to IBM.
Clinical Points
- Total excess costs in the civilian population represented 81.6% of the total economic burden of posttraumatic stress disorder (PTSD), yet previous literature mostly focused on the military population.
- The economic burden of PTSD goes beyond direct health care costs and rivals that of other costly mental health conditions.
- Increased awareness of PTSD and expansion of evidence-based interventions are warranted.
References (97)

- Bryant RA. Post-traumatic stress disorder: a state-of-the-art review of evidence and challenges. World Psychiatry. 2019;18(3):259–269. PubMed CrossRef
- Miloyan B, Bulley A, Bandeen-Roche K, et al. Anxiety disorders and all-cause mortality: systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. 2016;51(11):1467–1475. PubMed CrossRef
- Zivin K, Bohnert AS, Mezuk B, et al. Employment status of patients in the VA health system: implications for mental health services. Psychiatr Serv. 2011;62(1):35–38. PubMed CrossRef
- American Psychological Association. Clinical Practice Guideline for the Treatment of PTSD. American Psychological Association website. https://www.apa.org/ptsd-guideline/ptsd.pdf. 2017.
- Department of Veterans Affairs, Department of Defense. Clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder. US Dept of Veterans Affairs website. https://www.healthquality.va.gov/guidelines/mh/ptsd/. 2017. Accessed September 15, 2021.
- World Health Organization. Guidelines for the Management of Conditions Specifically Related to Stress. 2013. WHO website. https://apps.who.int/iris/bitstream/handle/10665/85119/9789241505406_eng.pdf. 2013. Accessed September 15, 2021.
- Meltzer EC, Averbuch T, Samet JH, et al. Discrepancy in diagnosis and treatment of post-traumatic stress disorder (PTSD): treatment for the wrong reason. J Behav Health Serv Res. 2012;39(2):190–201. PubMed CrossRef
- Stein MB, Rothbaum BO. 175 years of progress in PTSD therapeutics: learning from the past. Am J Psychiatry. 2018;175(6):508–516. PubMed CrossRef
- Kantor V, Knefel M, Lueger-Schuster B. Perceived barriers and facilitators of mental health service utilization in adult trauma survivors: a systematic review. Clin Psychol Rev. 2017;52:52–68. PubMed CrossRef
- Kazlauskas E. Challenges for providing health care in traumatized populations: barriers for PTSD treatments and the need for new developments. Glob Health Action. 2017;10(1):1322399. PubMed CrossRef
- Senneseth M, Alsaker K, Natvig GK. Health-related quality of life and post-traumatic stress disorder symptoms in accident and emergency attenders suffering from psychosocial crises: a longitudinal study. J Adv Nurs. 2012;68(2):402–413. PubMed CrossRef
- Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61(suppl 5):4–12, discussion 13–14. PubMed
- Seal KH, Cohen G, Waldrop A, et al. Substance use disorders in Iraq and Afghanistan veterans in VA healthcare, 2001–2010: implications for screening, diagnosis and treatment. Drug Alcohol Depend. 2011;116(1–3):93–101. PubMed CrossRef
- Chan D, Cheadle AD, Reiber G, et al. Health care utilization and its costs for depressed veterans with and without comorbid PTSD symptoms. Psychiatr Serv. 2009;60(12):1612–1617. PubMed CrossRef
- Ivanova JI, Birnbaum HG, Chen L, et al. Cost of post-traumatic stress disorder vs major depressive disorder among patients covered by medicaid or private insurance. Am J Manag Care. 2011;17(8):e314–e323. PubMed
- Surís A, Lind L, Kashner TM, et al. Sexual assault in women veterans: an examination of PTSD risk, health care utilization, and cost of care. Psychosom Med. 2004;66(5):749–756. PubMed CrossRef
- Walker EA, Katon W, Russo J, et al. Health care costs associated with posttraumatic stress disorder symptoms in women. Arch Gen Psychiatry. 2003;60(4):369–374. PubMed CrossRef
- Wang L, Li L, Zhou X, et al. A real-world evaluation of the clinical and economic burden of United States veteran patients with post-traumatic stress disorder. Value Health. 2016;19(7):A524. CrossRef
- Lehavot K, Katon JG, Chen JA, et al. Post-traumatic stress disorder by gender and veteran status. Am J Prev Med. 2018;54(1):e1–e9. PubMed CrossRef
- Wimalawansa S. Post-traumatic stress disorder: an under-diagnosed and under-treated entity. Comprehensive Research Journal of Medicine and Medical Science. 2013;1(1):1–12.
- Schein J, Houle C, Urganus A, et al. Prevalence of post-traumatic stress disorder in the United States: a systematic literature review. Curr Med Res Opin. 2021;37(12):2151–2161. PubMed CrossRef
- Agency for Healthcare Research and Quality. Mean expenditure per person with expense by insurance coverage, United States, 2017. Medical Expenditure Panel Survey. AHRQ website. https://meps.ahrq.gov/mepstrends/hc_use/. Accessed May, 13, 2020.
- Institute of Medicine. Board on the Health of Select Populations, & Committee on the Assessment of Ongoing Efforts in the Treatment of Posttraumatic Stress Disorder. Treatment for posttraumatic stress disorder in military and veteran populations: Final assessment. The National Academies Press website. https://www.nap.edu/catalog/18724/treatment-for-posttraumatic-stress-disorder-in-military-and-veteran-populations. 2014. Accessed May 15, 2020.
- Watkins KE, Pincus HA, Smith B, et al. Veterans Health Administration mental health program evaluation. US Dept of Veterans Affairs/RAND Health website. http://joiningforces.issuelab.org/resources/29966/29966.pdf. 2011. Accessed December 20, 2019.
- Wang PS, Lane M, Olfson M, et al. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):629–640. PubMed CrossRef
- Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93–100. PubMed CrossRef
- United States Department of Health & Human Services. Estimates of Funding for Various Research, Condition, and Disease Categories (RCDC). Research Portfolio Online Reporting Tools. NIH website. https://report.nih.gov/categorical_spending.aspx. 2019. Accessed October 3, 2019.
- National Center for PTSD. Fiscal Year 2018 Annual Report. National Center for PTSD website. https://www.ptsd.va.gov/about/work/docs/annual_reports/2018/NCPTSD_2018_Annual_Report_abridged.pdf. 2019. Accessed April 4, 2020.
- Sacks JJ, Gonzales KR, Bouchery EE, et al. 2010 national and state costs of excessive alcohol consumption. Am J Prev Med. 2015;49(5):e73–e79. PubMed CrossRef
- Substance Abuse and Mental Health Services Administration. Results from the 2018 National Survey on Drug Use and Health: Detailed Tables. SAMHSA website. http://www.samhsa.gov/data/release/2018-national-survey-drug-use-and-health-nsduh-releases. 2019. Accessed January 29, 2020.
- United States Department of Justice National Drug Intelligence Center. The economic impact of illicit drug use on American society. US Dept of Justice National Drug Intelligence Center website. https://www.justice.gov/archive/ndic/pubs44/44731/44731p.pdf. 2011. Accessed December 18, 2019.
- Han B, Olfson M, Huang L, et al. National trends in specialty outpatient mental health care among adults. Health Aff (Millwood). 2017;36(12):2062–2068. PubMed CrossRef
- Kaiser Family Foundation. Facilitating Access to Mental Health Services: A Look at Medicaid, Private Insurance, and the Uninsured. KFF website. https://www.kff.org/medicaid/fact-sheet/facilitating-access-to-mental-health-services-a-look-at-medicaid-private-insurance-and-the-uninsured/. 2017. Accessed January 17, 2020.
- Centers for Medicare and Medicaid Services. Physician Fee Schedule, 2018. CMS website. https://www.cms.gov/apps/physician-fee-schedule/search/search-results.aspx?Y=2&T=0&HT=0&CT=0&H1=90837&M=5. 2019. Accessed January 20, 2020.
- Tsai J. Lifetime and 1-year prevalence of homelessness in the US population: results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. J Public Health (Oxf). 2018;40(1):65–74. PubMed CrossRef
- United States Department of Housing and Urban Development. The 2018 annual homeless assessment report (AHAR) to Congress. Part 1: Point-in-time estimates of homelessness. HUD Exchange website. https://files.hudexchange.info/resources/documents/2018-AHAR-Part-1.pdf. 2018. Accessed January 15, 2020.
- Wong YLI, Park JM, Nemon H. Homeless service delivery in the context of continuum of care. Adm Soc Work. 2006;30(1):67–94. CrossRef
- O’Toole TP, Johnson EE, Borgia M, et al. Population-tailored care for homeless veterans and acute care use, cost, and satisfaction: a Prospective Quasi-Experimental Trial. Prev Chronic Dis. 2018;15:170311. PubMed CrossRef
- Social Security Administration. Master Beneficiary Record and Supplemental Security Record, 100 percent data: average monthly benefit, by sex and diagnostic group, December 2018 (in dollars). SSA website. https://www.ssa.gov/policy/docs/statcomps/di_asr/index.html. Accessed February 28, 2020.
- Hunter D, Boland R, Guerrera KM, et al. Analysis of Differences in Disability Compensation in the Department of Veterans Affairs. IDA website. https://www.va.gov/vetdata/docs/SurveysAndStudies/State_Variance_Study-Volumes_1_2.pdf. 2007. Accessed April 29, 2020.
- United States Department of Veterans Affairs. Annual Benefits Report FY 2018, Compensation. US Dept of Veterans Affairs website. https://www.benefits.va.gov/REPORTS/abr/docs/2018-compensation.pdf. 2018. Accessed May 5, 2020.
- United States Department of Veterans Affairs. Department of Veterans Affairs - Budget In Brief 2020. US Dept of Veterans Affairs website. https://www.va.gov/budget/products.asp. 2020. Accessed May 11, 2020.
- United States Census Bureau. Employment status 18 years and over by veteran status, age, and period of service, 2018 annual averages. Bureau of Labor Statistics website. https://www.bls.gov/news.release/archives/vet_03212019.htm. 2018. Accessed April 3, 2020.
- United States Census Bureau. Work Experience-People 15 Years Old and Over, by Total Money Earnings, Age, Race, Hispanic Origin, Sex, and Disability Status. US Census Bureau website. https://www.census.gov/data/tables/time-series/demo/income-poverty/cps-pinc/pinc-05.html#par_textimage_0. 2018. Accessed February 27, 2020.
- Ruggles S, Flood S, Goeken R, et al. IPUMS USA: Version 10.0 [dataset]. Minneapolis, MIN: IPUMS. IPUMS website. https://www.ipums.org/projects/ipums-usa/d010.v10.0 . 2020. Accessed April 30, 2020.
- Kessler RC, Frank RG. The impact of psychiatric disorders on work loss days. Psychol Med. 1997;27(4):861–873. PubMed CrossRef
- National Alliance for Caregiving. Caregiving in the US 2015. NAC and the AARP Public Institute. Washington DC: Greenwald & Associates. NAC website. https://www.caregiving.org/wp-content/uploads/2020/05/2015_CaregivingintheUS_Final-Report-June-4_WEB.pdf. 2015. Accessed February 18, 2020.
- National Alliance for Caregiving (NAC). On pins and needles: caregivers of adults with mental illness. NAC website. https://www.caregiving.org/wp-content/uploads/2020/05/NAC_Mental_Illness_Study_2016_FINAL_WEB.pdf. 2015. Accessed February 18, 2020.
- National Alliance on Mental Illness. Mental Health By the Numbers. NAMI website. https://www.nami.org/mhstats. 2019. Accessed April 16, 2020.
- United States Bureau of Labor Statistics. May 2018 National Occupational Employment and Wage Estimates United States. US Bureau of Labor Statistics website. https://www.bls.gov/oes/2018/may/oes_nat.htm. 2018. Accessed March 2, 2020.
- National Alliance for Caregiving. Caregivers of Veterans–Serving on the Homefront: Report of Study Findings. NAC website. https://www.caregiving.org/data/2010_Caregivers_of_Veterans_FULLREPORT_WEB_FINAL.pdf. 2010. Accessed May 6, 2020.
- Ramchand R, Tanielian T, Fisher MP, et al. Military Caregivers: Who are They? And Who Is Supporting Them? RAND website..https://www.rand.org/pubs/research_briefs/RB9764.html. 2014. Accessed April 28, 2020.
- Kochanek KD, Murphy SL, Xu J, et al. Deaths: Final Data for 2017. CDC website. https://stacks.cdc.gov/view/cdc/79486. 2019. Accessed October 14, 2019.
- United States Census Bureau. Employment Status 2018. US Census Bureau website. https://data.census.gov/cedsci/table?q=unemployment&hidePreview=true&tid=ACSST1Y2018.S2301&vintage=2018. 2018. Accessed February 11, 2020.
- United States Census Bureau. Current Population Survey, Annual Social and Economic Supplement, 2018. US Census Bureau website. https://www2.census.gov/programs-surveys/demo/tables/age-and-sex/2018/age-sex-composition/. 2019. Accessed February 18, 2020.
- United States Department of Veterans Affairs. National Center for Veterans Analysis and Statistics - Table 1L: VETPOP2016 LIVING VETERANS BY AGE GROUP, GENDER, 2015–2045. US Dept of Veterans Affairs website. https://www.va.gov/vetdata/veteran_population.asp. Accessed May 14, 2020.
- Robinson R. Cost-benefit analysis. BMJ. 1993;307(6909):924–926. PubMed CrossRef
- United States Department of Defense. Demographics Report: Profile of the Military Community. Military One Source website. https://www.militaryonesource.mil/data-research-and-statistics/military-community-demographics/2018-demographics-profile. 2018. Accessed May 14, 2020.
- United States Census Bureau. 2018 American Community Survey. US Census Bureau website. https://www.census.gov/data/tables/time-series/demo/health-insurance/acs-hi.html. 2019. Accessed January 15, 2020.
- United States Census Bureau. Employment Status, 2015 American Community Survey 1-year Estimates. https://data.census.gov/cedsci/table?q=employment%20status%202015%20american%20community%20survey&tid=ACSST1Y2015.S2301. Accessed January 18, 2017.
- Gates MA, Holowka DW, Vasterling JJ, et al. Posttraumatic stress disorder in veterans and military personnel: epidemiology, screening, and case recognition. Psychol Serv. 2012;9(4):361–382. PubMed CrossRef
- Purtle J. The legislative response to PTSD in the United States (1989–2009): a content analysis. J Trauma Stress. 2014;27(5):501–508. PubMed CrossRef
- Dutheil F, Mondillon L, Navel V. PTSD as the second tsunami of the SARS-Cov-2 pandemic. Psychol Med. 2021;51(10):1773–1774. PubMed
- Ni MY, Yao XI, Leung KSM, et al. Depression and post-traumatic stress during major social unrest in Hong Kong: a 10-year prospective cohort study. Lancet. 2020;395(10220):273–284. PubMed CrossRef
- Padhy SK, Sarkar S, Panigrahi M, et al. Mental health effects of climate change. Indian J Occup Environ Med. 2015;19(1):3–7. PubMed CrossRef
- Haller M, Chassin L. Risk pathways among traumatic stress, posttraumatic stress disorder symptoms, and alcohol and drug problems: a test of four hypotheses. Psychol Addict Behav. 2014;28(3):841–851. PubMed CrossRef
- National Center for Injury Prevention and Control. National Intimate Partner and Sexual Violence Survey. Data Brief - Updated Release; 2015.
- Kessler RC, Rose S, Koenen KC, et al. How well can post-traumatic stress disorder be predicted from pre-trauma risk factors? an exploratory study in the WHO World Mental Health Surveys. World Psychiatry. 2014;13(3):265–274. PubMed CrossRef
- American Heart Association. Cardiovascular Disease: A Costly Burden for America Projections Through 2035. American Heart Association website. https://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_491543.pdf. 2017.
- Cloutier M, Aigbogun MS, Guerin A, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77(6):764–771. PubMed CrossRef
- Cloutier M, Greene M, Guerin A, et al. The economic burden of bipolar I disorder in the United States in 2015. J Affect Disord. 2018;226:45–51. PubMed CrossRef
- Compton WM, Conway KP, Stinson FS, et al. Changes in the prevalence of major depression and comorbid substance use disorders in the United States between 1991–1992 and 2001–2002. Am J Psychiatry. 2006;163(12):2141–2147. PubMed CrossRef
- DuPont RL, Rice DP, Miller LS, et al. Economic costs of anxiety disorders. Anxiety. 1996;2(4):167–172. PubMed CrossRef
- Adler L, Childress A, Cloutier M, et al. Economic burden of attention-deficit/hyperactivity disorder (ADHD) among adults in the United States: a societal perspective. Value Health. 2021;24:S128. CrossRef
- Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. 2021;39(6):653–665. PubMed CrossRef
- Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3(2):171–178. PubMed CrossRef
- Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. PubMed CrossRef
- Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. 2017;143(8):783–822. PubMed CrossRef
- Krystal JH, Davis LL, Neylan TC, et al. It is time to address the crisis in the pharmacotherapy of posttraumatic stress disorder: a consensus statement of the PTSD Psychopharmacology Working Group. Biol Psychiatry. 2017;82(7):e51–e59. PubMed CrossRef
- Cohen GH, Tamrakar S, Lowe S, et al. Comparison of simulated treatment and cost-effectiveness of a stepped care case-finding intervention vs usual care for posttraumatic stress disorder after a natural disaster. JAMA Psychiatry. 2017;74(12):1251–1258. PubMed CrossRef
- Le QA, Doctor JN, Zoellner LA, et al. Cost-effectiveness of prolonged exposure therapy versus pharmacotherapy and treatment choice in posttraumatic stress disorder (the Optimizing PTSD Treatment Trial): a doubly randomized preference trial. J Clin Psychiatry. 2014;75(3):222–230. PubMed CrossRef
- Sloan DM, Marx BP. Written Exposure Therapy for PTSD: A Brief Treatment Approach for Mental Health Professionals. American Psychological Association; 2019.
- Bremner JD, Southwick SM, Darnell A, et al. Chronic PTSD in Vietnam combat veterans: course of illness and substance abuse. Am J Psychiatry. 1996;153(3):369–375. PubMed CrossRef
- Hawn SE, Cusack SE, Amstadter AB. A systematic review of the self-medication hypothesis in the context of posttraumatic stress disorder and comorbid problematic alcohol use. J Trauma Stress. 2020;33(5):699–708. PubMed CrossRef
- Pietrzak RH, Goldstein RB, Southwick SM, et al. Prevalence and Axis I comorbidity of full and partial posttraumatic stress disorder in the United States: results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J Anxiety Disord. 2011;25(3):456–465. PubMed CrossRef
- GBD 2016 Alcohol and Drug Use Collaborators. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. 2018;5(12):987–1012. PubMed CrossRef
- National Institute on Drug Abuse. Costs of Substance Abuse. National Institute on Drug Abuse website. https://www.drugabuse.gov/drug-topics/trends-statistics/costs-substance-abuse. 2020. Accessed October 2, 2020.
- Drake RE, Skinner JS, Bond GR, et al. Social Security and mental illness: reducing disability with supported employment. Health Aff (Millwood). 2009;28(3):761–770. PubMed CrossRef
- Goldberg RW, Lucksted A, McNary S, et al. Correlates of long-term unemployment among inner-city adults with serious and persistent mental illness. Psychiatr Serv. 2001;52(1):101–103. PubMed CrossRef
- Henkel D. Unemployment and substance use: a review of the literature (1990–2010). Curr Drug Abuse Rev. 2011;4(1):4–27. PubMed CrossRef
- Gradus JL. Posttraumatic stress disorder and death from suicide. Curr Psychiatry Rep. 2018;20(11):98. PubMed CrossRef
- LeBouthillier DM, McMillan KA, Thibodeau MA, et al. Types and number of traumas associated with suicidal ideation and suicide attempts in PTSD: findings from a US nationally representative sample. J Trauma Stress. 2015;28(3):183–190. PubMed CrossRef
- McKinney JM, Hirsch JK, Britton PC. PTSD symptoms and suicide risk in veterans: serial indirect effects via depression and anger. J Affect Disord. 2017;214:100–107. PubMed CrossRef
- Pompili M, Sher L, Serafini G, et al. Posttraumatic stress disorder and suicide risk among veterans: a literature review. J Nerv Ment Dis. 2013;201(9):802–812. PubMed CrossRef
- Making the Case for IPS Supported Employment. IPS website. https://ipsworks.org/wp-content/uploads/2017/08/Making-the-case-for-IPS.pdf. 2017. Accessed January 8, 2021.
- Davis LL, Kyriakides TC, Suris AM, et al; VA CSP #589 Veterans Individual Placement and Support Toward Advancing Recovery Investigators. Effect of evidence-based supported employment vs transitional work on achieving steady work among veterans with posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. 2018;75(4):316–324. PubMed CrossRef
- Mueller L, Wolfe WR, Neylan TC, et al. Positive impact of IPS supported employment on PTSD-related occupational-psychosocial functional outcomes: results from a VA randomized-controlled trial. Psychiatr Rehabil J. 2019;42(3):246–256. PubMed CrossRef
This PDF is free for all visitors!