Abstract
Objective: To test esmethadone (REL-1017) as adjunctive treatment in patients with major depressive disorder (MDD) and inadequate response to standard antidepressants.
Methods: In this phase 3, double-blind, placebo-controlled trial, outpatients with MDD (DSM-5) were randomized to daily oral esmethadone (75 mg on day 1, followed by 25 mg daily on days 2 through 28) or placebo between December 2020 and December 2022. The primary efficacy measure was change from baseline (CFB) to day 28 in the Montgomery-Asberg Depression Rating Scale (MADRS) score. The intent-to-treat (ITT) population included all randomized participants. The per-protocol (PP) population included completers without major protocol deviations impacting assessment. Post hoc analyses included participants with severe depression (baseline MADRS score ≥35).
Results: For the ITT analysis (n = 227), mean CFB was 15.1 (SD 11.3) for esmethadone (n = 113) and 12.9 (SD 10.4) for placebo (n = 114), with a mean difference (MD) of 2.3, which was not statistically significant (P = .154; Cohen effect size [ES] = 0.21). Remission rates were 22.1% and 13.2% (P = .076), and response rates were 39.8% and 27.2% (P = .044) with esmethadone and placebo, respectively. For the PP analysis (n = 198), mean CFB was 15.6 (SD 11.2) for esmethadone (n = 101) and 12.5 (SD 9.9) for placebo (n = 97), with an MD of 3.1 (P = .051; ES =0.29). In post hoc analyses of patients with baseline MADRS ≥35 in the ITT population (n = 112), MD was 6.9; P = .0059; ES = 0.57, and for the PP population (n = 98), MD was 7.9; P = .0015; ES = 0.69. Adverse events (AEs) were predominantly mild or moderate and transient, with no significant differences between groups.
Conclusions: The primary end point was not met. Esmethadone showed stronger efficacy in PP than in ITT analyses, with the discrepancy not attributable to AEs impacting treatment adherence. Significant efficacy occurred in post hoc analyses of patients with severe depression. Esmethadone was well tolerated, consistent with prior studies.
Trial Registration: ClinicalTrials.gov identifier: NCT04688164
J Clin Psychiatry 2024;85(3):24m15265
Author affiliations are listed at the end of this article.
Major depressive disorder (MDD) is the second leading cause of disability and chronic disease burden in the United States, as measured by disability-adjusted life years.1 Data from the National Epidemiologic Survey on Alcohol and Related Conditions-III demonstrate a 12-month and lifetime prevalence of MDD of 10.4% and 20.6%, respectively.2 Approximately 50%–60% of patients with MDD do not achieve an adequate response following the first antidepressant treatment.3 Depressed patients with an inadequate response to antidepressant therapy contribute a disproportionately high burden of illness compared to patients who respond to treatment.
The neurobiology of MDD is progressively disengaging from the classic serotonergic hypothesis,4 and the risk-benefit ratio of available antidepressants, which mostly target monoaminergic neurotransmissions, has been questioned.5 Alternative hypotheses for the neurobiology of MDD implicate impairment of neural plasticity.6–8 The pivotal role of N-methyl-D-aspartate receptors (NMDARs) in neural plasticity is well established,9,10 and dysregulation of glutamatergic signaling via NMDARs is increasingly recognized as a potential pathological mechanism for neuropsychiatric disorders and a target for novel antidepressants.11–19 Uncompetitive NMDAR antagonists have been approved by the Food and Drug Administration (FDA) for treating MDD. Intranasal esketamine has been FDA-approved for treatment-resistant depression (TRD) and for MDD with suicidal ideation; the oral twice daily dextromethorphan-bupropion combination has been approved for MDD. Recently, in silico and in vitro studies have advanced our understanding of the interactions of uncompetitive NMDAR antagonists and NMDARs20,21 and the comparative pharmacological affinity and activity of different NMDAR uncompetitive antagonists.21 Experimental models of depressive like behavior suggest that NMDAR uncompetitive antagonists may improve depressive-like behavior via brain-derived neurotrophic factor–dependent restoration of neural plasticity.11,12,15,17,19 Recent reviews indicate that NMDAR uncompetitive antagonists, including esmethadone (REL-1017), are at the forefront among novel antidepressant candidates.13,14,18
Esmethadone is a novel NMDAR uncompetitive antagonist antidepressant candidate with promising safety, tolerability, and efficacy results from phase 1 and phase 2 trials.22,23 In phase 1 studies, oral esmethadone was found to be safe and well tolerated at doses up to 150 mg, nausea and vomiting limited the use of higher doses, and oral esmethadone exhibits linear pharmacokinetics with dose proportionality.22 A phase 2 study with adjunctive oral once daily esmethadone confirmed the safety and tolerability seen in phase 1 and showed rapid and robust efficacy.23
Chiral configuration is known to impart opioid activity to racemic opioid molecules; as a rule, after chiral separation, only one of the two chiral opioid enantiomers retains meaningful opioid agonist activity.24–26 Esmethadone, the dextro-isomer of racemic methadone, is a low affinity, low-potency NMDAR uncompetitive antagonist that binds to the phencyclidine site of the NMDAR at low-micromolar half-maximal inhibitory concentrations (IC50).25,27 Esmethadone has 20- to 40-fold lower affinity for mu opioid receptors compared with levomethadone28,29 and does not contribute in a meaningful way to the opioid effects of racemic methadone, which are a result of its enantiomer, levomethadone.24–26,30–32 Esmethadone may even act as an opioid antagonist within the racemic mixture, attenuating the opioid agonist effects of levomethadone.32,33 Preclinical studies showed lack of self administration in animal models predictive of abuse potential.31,32 Clinical studies in recreational substance users showed that tested doses of esmethadone up to 150 mg were statistically equivalent to placebo.34 These recent state-of-the-art studies to define abuse potential confirm prior literature indicating that esmethadone has no meaningful opioid agonist activity and no meaningful abuse potential.31,32,34
In addition to opioid affinity and NMDAR affinity, esmethadone inhibits serotonin and norepinephrine transporters, with affinities in the micromolar range that are approximately 500-fold (serotonin transporters) and 100-fold (norepinephrine transporters) lower than those seen for duloxetine.29,35 These 100-plus fold differences in IC50 compared with duloxetine suggest that a primary monoaminergic antidepressant mechanism of action for esmethadone is unlikely. Preclinical studies and the ongoing clinical use of NMDAR antagonists are advancing our understanding of the neurobiology of MDD. 9,16,17,19,36,37 Esmethadone appears to have preferential activity on GluN2D subtypes, an NMDAR subtype implicated in MDD, triggered by chronic excitotoxicity at resting membrane potential.37
Leaving aside the mechanism of action, oral once daily esmethadone showed efficacy in a phase 2 trial and confirmed a favorable tolerability and safety profile across multiple clinical studies without any signal for the metabolic, cardiovascular, and neurological side effects seen with atypical antipsychotic drugs currently approved as adjunctive treatment of MDD.22,23 Esmethadone does not cause Olney lesions in rats,38 a potential indicator of its safety compared to other uncompetitive NMDAR antagonists. Long-term human exposure to esmethadone in millions of patients treated for over half a century with racemic S-R-methadone for opioid use disorder and pain, generally at doses higher than the doses proposed for MDD, has been safe overall. We therefore evaluated the efficacy, safety, and tolerability of esmethadone in a phase 3 study of patients with MDD unresponsive to monoaminergic antidepressants.
METHODS
This multicenter trial was conducted in accordance with the International Council on Harmonization guidelines for Good Clinical Practice, the principles of the Declaration of Helsinki, and all regulatory requirements. The study protocol was reviewed and approved by an institutional review board, and written informed consent was obtained from all participants after receiving a complete description of the study and prior to any study procedure.
Study Design
This was a 28-day double-blind, placebo-controlled, randomized phase 3 trial conducted in 43 centers in the United States from December 2020 to December 2022. The overall duration of the trial, including the screening period, was approximately 58 days (Supplementary Figure 1). During the screening period, clinicians from the Massachusetts General Hospital Clinical Trials Network and Institute (MGH-CTNI) independently assessed prior antidepressant treatment response and history using the MGH Antidepressant Treatment Response Questionnaire (ATRQ). Raters from the sites were required to obtain certification and training prior to rating study participants. The screening and rater review process are presented in Supplementary Appendix 1.
Participants
Adult patients ages 18–65 years were eligible if they met criteria for MDD defined by Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 criteria), if they had a 17-item Hamilton Depression Rating Scale (HAM-D)39 score ≥19 and did not show an increase in absolute value of >40% or a decrease >20% on the HAM-D score between screening and baseline, and if they had a body mass index (BMI) between 18 and 30 kg/m2. Patients also had a current major depressive episode lasting 8 weeks to 36 months and had an inadequate response from 1–3 courses of antidepressant treatment during the same episode, as determined by a clinician from the MGH-CTNI who independently assessed each patient using the MGH ATRQ. Patients were required to have a Montgomery Asberg Depression Rating Scale (MADRS) total score40 at baseline ≥24 points. Patients were taking the same SSRI, serotonin-norepinephrine reuptake inhibitor, or bupropion for at least 8 weeks prior to screening and maintained the same adequate dose for the last 4 weeks. Exclusion criteria included use of opioids, anxiolytics, antipsychotics, anticonvulsants, mood stabilizers, stimulants, NMDAR antagonists, electroconvulsive therapy, vagus nerve stimulation, or repetitive transcranial magnetic stimulation. Any medication taken consistently by the patient for 30 days prior to screening that was not a prohibited medication was continued during the trial (see Supplementary Table 1 for list of prohibited medications). Initiation of medications during the trial was not allowed. Patients at risk for suicide and patients with history of bipolar disorder, psychosis or mania, substance use disorder or heavy alcohol use, and patients with positive results on urine test for alcohol or illicit drugs also were excluded. For a full list of inclusion/exclusion criteria, please see Supplementary Appendix 2.
Procedures
Patients were randomized by an unblinded pharmacist through an interactive web response system in a 1:1 ratio to esmethadone or placebo. The randomization code used in the interactive web response system was prepared by a statistician who was not involved in the study. On day 1, patients received a loading dose of esmethadone 75 mg or placebo. The loading dose of esmethadone was computed based on pharmacokinetic data from a phase 1 study22 to achieve steady-state concentrations by day 1. Oral 75 mg esmethadone is well tolerated without evidence of subjective effects in healthy volunteers,22 in patients with MDD,23 or in recreational substance users,34 making unblinding unlikely. On days 2–28, patients received esmethadone 25 mg or placebo. The first 200 patients underwent a 2-week safety-withdrawal assessment after discontinuation of study medication. Safety assessments included evaluation of frequency and severity of adverse events (AEs), and changes in clinical laboratory tests (chemistry, hematology, and urinalysis), electrocardiogram, physical examination, vital signs (blood pressure, heart rate, and respiratory rate), weight, and body temperature. Other safety assessments included suicidal ideation and behavior with the Columbia Suicide Severity Rating Scale (C-SSRS; a higher score indicates a higher intensity of suicidal ideation)41; present state dissociative symptoms with the Clinician Administered Dissociative States Scale (CADSS; a higher score indicates a higher likelihood of the presence of a dissociative state)42; and psychotic symptoms with the 4-item Positive Symptom Rating Scale.43 “Drug liking,” “drug high,” and “desire to take the drug again” were assessed with a 100-point visual analog scale (VAS). The Misuse, Abuse, and Diversion Drug Event Reporting System (MADDERS)44 was used to assess potentially abuse-related events. Potential withdrawal was assessed for 14 days after abrupt treatment discontinuation (days 28–42) using the Physician Withdrawal Checklist (PWC),45 Clinical Opiate Withdrawal Scale (COWS),46 and Subjective Opiate Withdrawal Scale (SOWS).47 Abuse-related AEs were defined as AEs of special interest.
Outcomes
The primary efficacy end point was the mean change from baseline (CFB) to day 28 for the MADRS total score. Remission (MADRS total score ≤10) and response (≥50% MADRS improvement from baseline) were key secondary end points.
Statistical Analysis
The study was designed to achieve 90% power, with an overall 2-tailed alpha level of 0.05. The sample size was estimated based on a Cohen effect size (ES) assumption of 0.45 in the main estimand of the primary efficacy end point, defined as the absolute CFB to day 28 in the MADRS total score. Using the treatment policy for intercurrent events, a net sample size of 210 complete patients was estimated, which corresponded to approximately 220 randomized participants considering an early termination rate of 5%. The sample size of 210 total completers was computed using a 2-sided t-test assuming equal variances. The assumed ES was determined by taking a conservative approach from analysis of a phase 2 study23 and considering studies of adjunctive treatment of MDD with brexpiprazole48 and esketamine.49,50 Sample size calculations were performed with the software package nQuery 8, version 8.5.2.0.
The intent-to-treat (ITT) population included all randomized patients. The prespecified supportive analysis was the per-protocol (PP) population, which included all patients completing the 28-day treatment period without major protocol deviations impacting efficacy assessments. A post hoc analysis was performed in patients with severe depression, defined as baseline MADRS ≥35. The safety population comprised all randomized patients who received any dose of study drug and coincided with the ITT. Data for the primary end point were analyzed using mean difference (MD) in MADRS total score and using a mixed-effect model with repeated measures (MMRM), with consideration of repeated assessments of the MADRS 10 total score and with the independent variables of treatment, visit, the interaction of treatment and visit, and baseline MADRS total score. Comparisons of response rate and remission rate were analyzed using 95% CI for MD (Wilson confidence limits), χ2 test (2-sided with α = 0.05), and odds ratio (OR) with 95% CI.
RESULTS
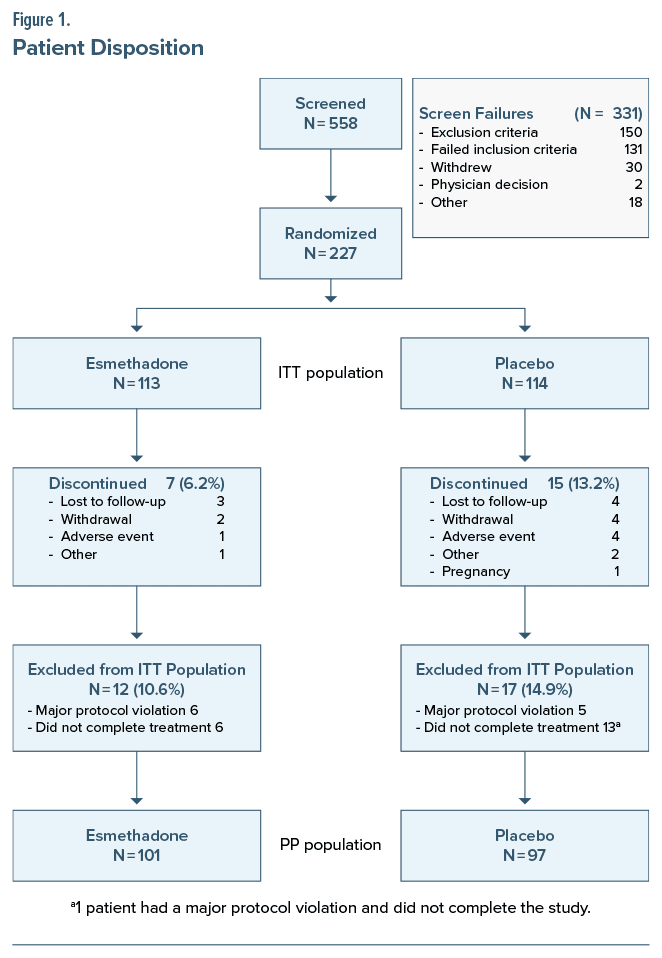
The ITT population comprised 227 randomized patients. The PP population comprised 198 patients completing treatment without major protocol deviations affecting efficacy assessments (Figure 1). Among the 29 patients included in the ITT population who were excluded pre-database lock from the PP analysis (17 placebo and 12 esmethadone), 19 patients (13 placebo and 6 esmethadone) did not complete treatment, and 11 patients (5 placebo and 6 esmethadone) had major protocol deviations affecting treatment outcome (1 patient did not complete treatment and had a major protocol deviation).
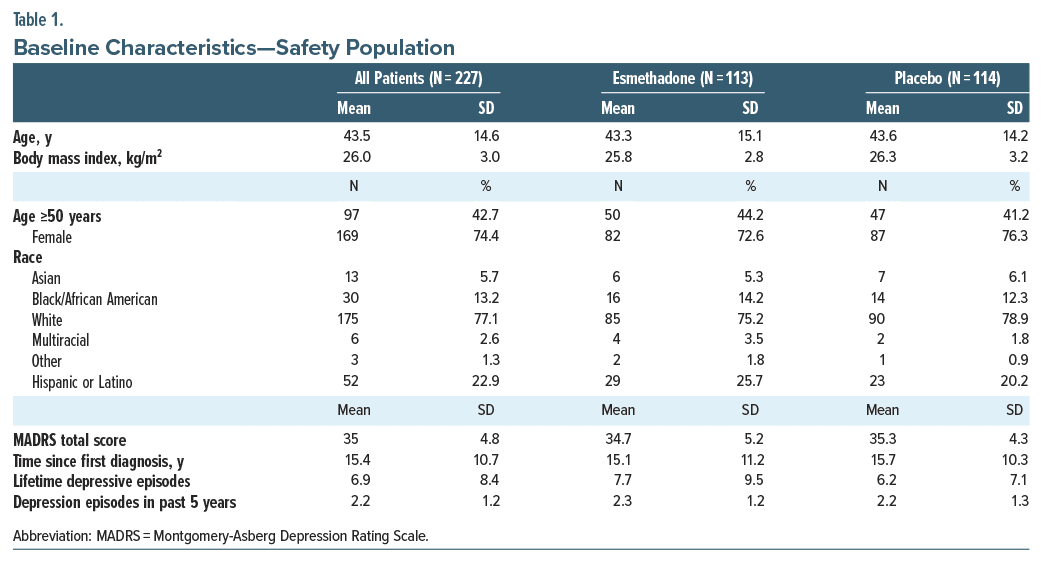
Patients in the esmethadone and placebo groups were generally comparable for baseline demographic and clinical characteristics (Table 1). Mean (SD) age was 43.5 (14.6) years, 74% were female, and 77% were white. Mean baseline MADRS score was 35.0 (4.8), and approximately 50% of patients (112/227) has a baseline MADRS score of ≥35, indicating severe depression. Mean (SD) duration of the current major depressive episode was 1.2 (2.2) years. Patients had an average of 6.9 (8.4) lifetime major depressive episodes and an average of 15.4 (10.7) years since the first MDD diagnosis, indicating that most patients had a long history of depression.
Efficacy
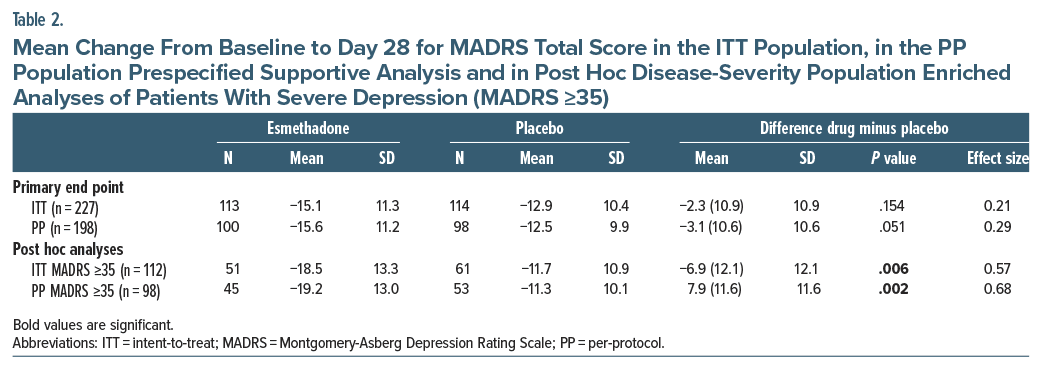
For the primary end point in the ITT population, mean (SD) CFB to day 28 for the MADRS total score was 15.1 (11.3) for esmethadone (n=113) and 12.9 (10.4) for placebo (n=114) (MD: 2.3 (10.9); P =.154; ES=0.21 (Table 2, Figure 2A). In the PP population, mean (SD) CFB for MADRS was 15.6 (11.2) for esmethadone (n=101) and 12.5 (9.9) for placebo (n= 97) (MD: 3.1 (10.6); P =.051; ES=0.29) (Figure 2B).
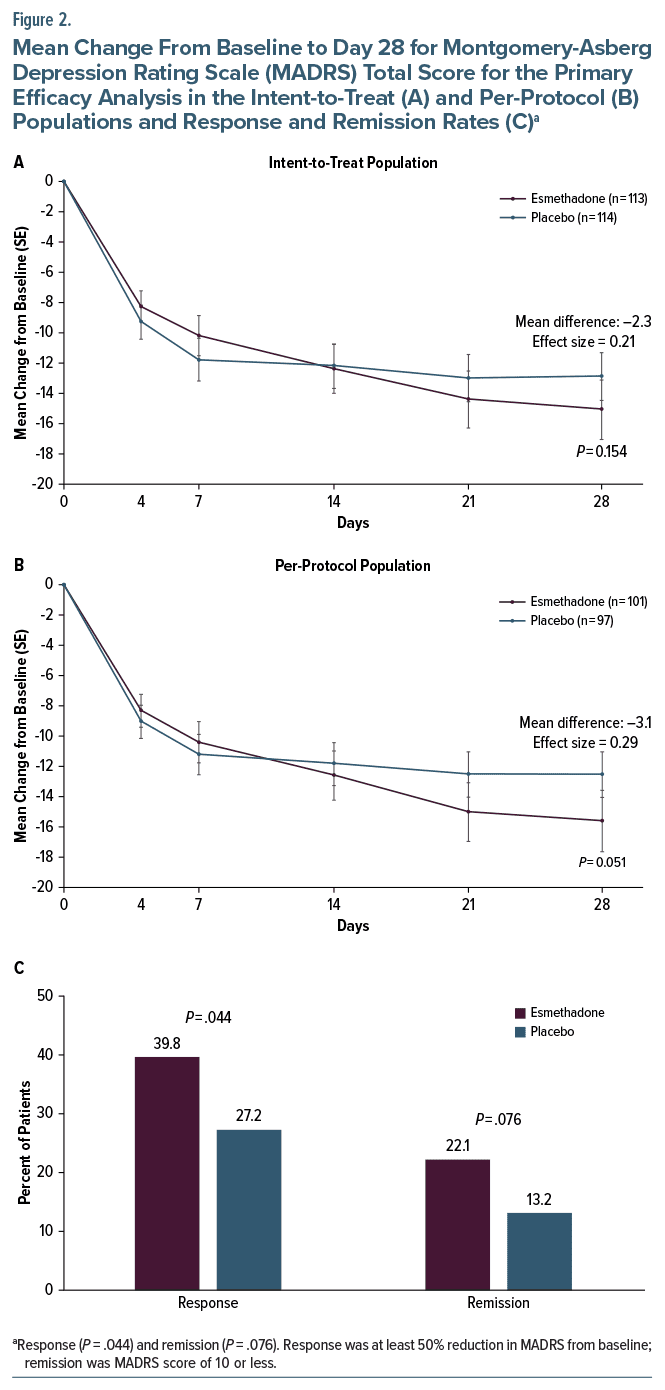
Remission rate at day 28 was 22.1% with esmethadone and 13.2% with placebo (MD: 9.0%, 95% CI, −0.9 to 18.8; P=.076; OR: 1.88, 95% CI, 0.88 to 4.08). Response rate was 39.8% with esmethadone and 27.2% with placebo (MD: 12.6%, 95% CI, 0.5 to 24.8; P =.044; OR: 1.77, 95% CI, 0.98 to 3.23) (Figure 2C). In the PP population, remission rates at day 28 were 23.8% and 13.4% (P=.062), and response rates were 42.6% and 29.9% (P=.064) for esmethadone and placebo, respectively.
In post hoc analyses of patients with severe depression (MADRS score ≥35 at baseline), significant improvement occurred with esmethadone vs. placebo in both the ITT and PP populations (MD CFB 6.9 and 7.9; P = .0059 and P = .0015; ES = 0.57 and 0.68, respectively) (Table 2 and Figure 3). In this post hoc disease-severity population analysis, remission rates at day 28 were 27.5% and 11.5% (MD: 16.0%, 95% CI, 1.3 to 30.6; P = .031), and response rates at day 28 were 43.1% and 21.3% (MD: 21.8%, 95% CI, 4.8 to 38.9; P = .013) for esmethadone and placebo, respectively, in the ITT population. Remission rates were 28.9% and 11.3% (MD: 17.6%, 95% CI, 1.8 to 33.3; P = .028), and response rates were 46.7% and 22.6% (MD: 24.0%, 95% CI, 5.6 to 42.4; P = .012) for esmethadone and placebo, respectively, in the PP population.
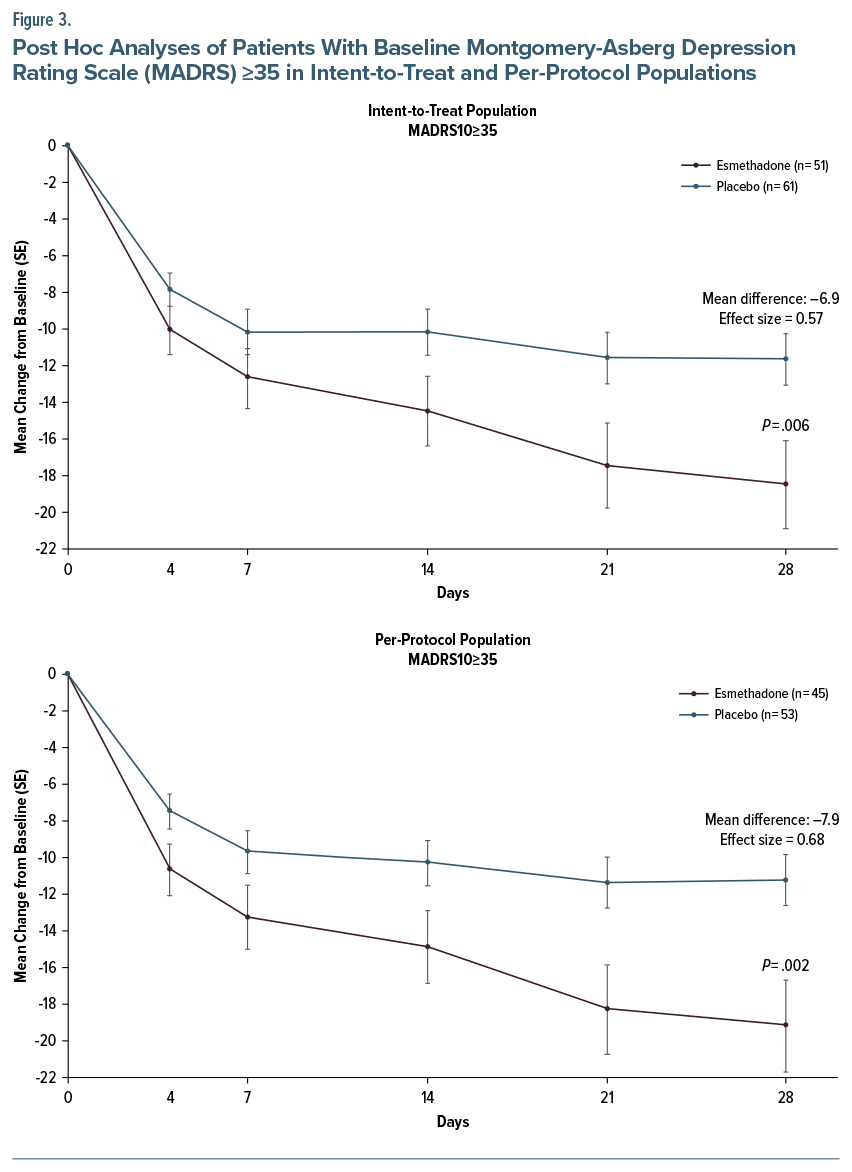
The MMRM analysis for the ITT, PP, and post hoc severe depression populations showed significant differences between esmethadone and placebo only for the severe population with ES of 0.51 and 0.64 for the ITT and PP populations (Supplementary Table 2).
Safety and Tolerability
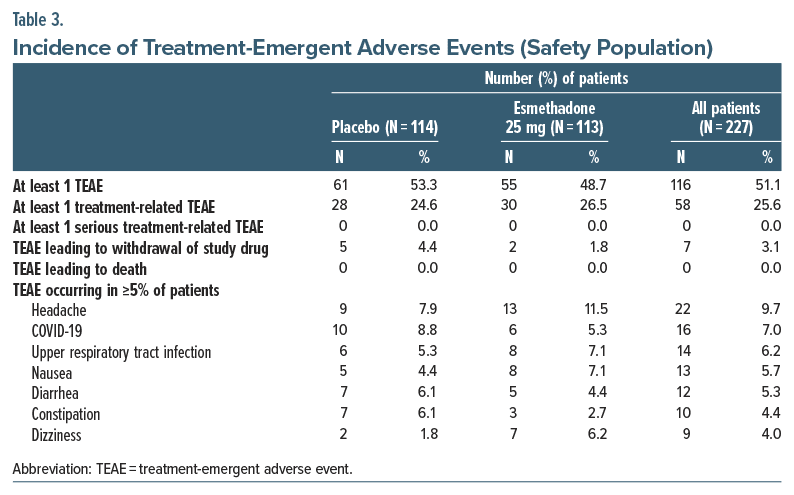
The incidence of treatment-emergent adverse events (TEAEs) was comparable between esmethadone and placebo (Table 3). No serious AEs or deaths related to study treatment were reported. Seven patients discontinued study treatment due to AEs (5 placebo [anxiety, depression, panic attack, pregnancy, throat irritation, pruritus, urticaria] and 2 esmethadone [suicidal ideation, nausea, dizziness]). AEs were predominantly mild or moderate and transient. The most common TEAEs were headache, COVID-19, dizziness, and gastrointestinal complaints. There were 3 unrelated or unlikely related serious AEs in the esmethadone group.
No clinically significant findings were observed with esmethadone for vital signs, body weight/BMI, or clinical laboratory testing. For the esmethadone group, mean (SD) weight and BMI were 72.5 (11.0) kg and 25.8 (7.8) kg/m2 at baseline and 73.0 (10.8) kg and 26.0 (2.7) kg/m2 at end of treatment; for the placebo group, mean (SD) weight and BMI were 73.8 (13.2) kg and 26.3 (3.2) kg/m2 at baseline and 75.4 (14.5) kg and 26.8 (3.4) kg/m2 at end of treatment. One patient with esmethadone had an increase in alanine aminotransferase levels >3 times upper limit of normal, and 2 patients with esmethadone had an increase in aspartate aminotransferase levels >3 times upper limit of normal. These events were attributed to viral illness and use of acetaminophen in 1 patient, to HIV medications in 1 patient, and to excessive physical exercise in 1 patient. These 3 AEs were considered unlikely related to esmethadone. No abnormal liver function tests occurred with placebo. Mean (SD) CFB to day 28 for the QT interval with Fridericia correction (QTcF) interval was 0.24 (13.5) ms for esmethadone and −3.1 (11.9) ms for placebo. Analysis of worst CFB at any time point for the QTcF interval showed no QTcF increase ≥60 ms and no QTcF >480 ms with either esmethadone or placebo. No differences between esmethadone and placebo were observed for shifts from baseline to worst value on the C-SSRS. No signal of abuse potential was observed from CADSS and VAS, and no signal for withdrawal was seen on PWC, COWS, or SOWS. No cases of withdrawal, misuse, abuse, or diversion were recorded in MADDERS. In this study, mean esmethadone end-of-dose concentration at steady state day 7 was 192 ng/mL.
DISCUSSION
Approximately 50%–60% of patients with MDD fail to achieve an adequate response following their first antidepressant treatment.3 These patients are left with few satisfactory pharmacological options. Several atypical antipsychotics are FDA-approved for the treatment of depressed patients with inadequate response to first-line antidepressant therapy. However, atypical antipsychotics carry significant neurological, cardiovascular, and metabolic side effects.51–53 No NMDAR antagonists are FDA-approved as adjunctive treatment for MDD. Intranasal esketamine, approved for MDD with acute suicidal ideation and TRD, has limitations due to dissociative and psychotomimetic effects requiring clinical supervision.54 The oral twice daily dextromethorphan-bupropion combination has been approved for MDD.
In this multicenter trial, esmethadone did not meet the primary efficacy end point in the ITT analysis (MD=2.3; P=.154; ES=0.21). However, esmethadone showed a statistically significant improvement in response rate compared to placebo (P=.044) and an encouraging nonsignificant trend for improvement in remission rate (P=.076). In the PP prespecified supportive analysis, results trended toward a more favorable outcome (MD=3.1; P =.051; ES=0.29). In this trial, the difference in efficacy between ITT and PP analyses is attributed to the exclusion of patients with protocol noncompliance due to reasons other than esmethadone-related AEs. The 29 patients who were not compliant with the protocol and were not included in the PP analysis are unlikely to inform on treatment efficacy, suggesting that in this study, the PP analysis of compliant patients may have provided an enhanced measure of efficacy.55,56 Arguably, if the sample size calculation had been based on more widely accepted assumed ES for standard antidepressants, ie, ES around 0.3,57 the trial may have potentially met its primary end point. Furthermore, in the analyzed populations (ITT, PP, severe depression population), the esmethadone-treated groups had a slope that was still declining at the conclusion of the 4-week treatment period, potentially suggesting that a longer study may have led to enhanced separation from placebo.
No biomarker consistently improves the accuracy of MDD diagnosis, and according to DSM-5 criteria, the assessment of severity is critical for diagnosis. A MADRS score of 35 or more indicates severe depression and may enhance diagnostic accuracy. We hypothesize that in this study, the subgroup of patients with severe depression may have included a lower number of patients with transient reactive depression and a lower number of “professional patients,”58–60 thus explaining the favorable results seen in the severity-enriched post hoc analysis.
Adverse events were mild or moderate and transient and were comparable in the two groups. No treatment-related serious AEs were observed. No withdrawal effects and no signals of potential abuse were observed on a broad battery of specialized measurements, confirming the lack of meaningful abuse potential seen in ad hoc studies.34 The effects on QT prolongation in these patients with MDD and concomitant antidepressants were mild and consistent with prior results23 and with results seen in drug-free healthy volunteers.22
This study may have been underpowered relative to other antidepressant trials,61 and the 4-week treatment course may not have captured the full therapeutic effect of esmethadone. The safety/tolerability profile was consistent with previous phase 1 and phase 2 studies.
CONCLUSION
While neither the primary efficacy end point nor the secondary end point of remission was achieved, the statistically significant difference in the key secondary end point of response rate and results in the prespecified supportive PP analysis suggest meaningful antidepressant effects of esmethadone. Post hoc analyses of patients with severe MDD showed statistically significant efficacy with robust ES, consistent with results seen in the phase 2 trial.23 The overall results from this study strengthen prior evidence for the efficacy, safety, and tolerability of esmethadone as a promising antidepressant for the adjunctive treatment of MDD.22,23,34 The side effect profile of esmethadone compares favorably with the side effects of the currently FDA-approved adjunctive treatments for MDD. Further phase 3 studies will better characterize the potential efficacy of esmethadone as adjunctive treatment in patients with persistent MDD despite ongoing treatment with adequate doses of standard antidepressants.
Article Information
Published Online: June 17, 2024. https://doi.org/10.4088/JCP.24m15265
© 2024 Physicians Postgraduate Press, Inc.
Submitted: January 16, 2024; accepted March 25, 2024.
To Cite: Fava M, Stahl SM, Pani L, et al. Efficacy and safety of esmethadone (REL-1017) in patients with major depressive disorder and inadequate response to standard antidepressants: a phase 3 randomized controlled trial. J Clin Psychiatry. 2024;85(3):24m15265.
Author Affiliations: Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts (Fava, Guidetti); Department of Psychiatry and Neuroscience, University of California Riverside, Riverside, California (Stahl); Department of Psychiatry, University of California San Diego, San Diego, California (Stahl); Relmada Therapeutics, Inc, Coral Gables, Florida (Pani, Kröger, Champasa, O’Gorman, Traversa, Inturrisi, Manfredi, Pappagallo); Department of Psychiatry and Behavioral Sciences, School of Medicine, University of Miami, Miami, Florida (Pani); Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy (Pani); Department of Pharmaceutical and Pharmacological Sciences, University of Padua, Padua, Italy (De Martin, Mattarei); Department of Psychiatry, SUNY Upstate Medical University, Syracuse, New York (Cutler); Neuroscience Education Institute, Carlsbad, California (Cutler); Department of Psychiatry/Behavioral Science, University of South Carolina School of Medicine, Greenville, South Carolina (Maletic); Consultant in Pharmaceutical Medicine, Kansas City, Missouri (Gorodetzky); Friends Research Institute, Baltimore, Maryland (Vocci); The Drug and Chemical Advisory Group LLC, Fairfax, Virginia (Sapienza); Baylor College of Medicine, MD Anderson Cancer Center, University of Houston, Houston, Texas (Kosten); Child Neuropsychiatry Unit, Department of Neuroscience, IRCCS Bambino Gesù Pediatric Hospital, Rome, Italy (Guidetti); Department of Health Sciences and Technology, ETH Zurich, Zurich, Switzerland (Alimonti); Department of Pharmaceutical and Pharmacological Sciences, and Department of Biomedical Sciences, University of Padua, Padua, Italy (Comai); Department of Psychiatry, McGill University, Montreal, Quebec, Canada (Comai); Department of Health Sciences, University of Milan, Milan, Italy (Folli); Cytel, Inc, Waltham, Massachusetts (Bushnell).
Corresponding Author: Paolo L. Manfredi, MD, Relmada Therapeutics, 2222 Ponce de Leon Blvd Floor 3, Coral Gables, FL 33134 ([email protected]).
Drs Pappagallo and Manfredi contributed equally.
Author Contributions: The listed authors made contributions in each of these 4 areas: (1) conception and design or data analysis and interpretation; (2) drafting of the manuscript or revision for important intellectual content; (3) approving the final version of the manuscript that is to be published; and (4) accountability for all aspects of the work and the ability to identify the contributions of each coauthor and ensure the integrity of their contributions.
Relevant Financial Relationships: Drs De Martin, Guidetti, Alimonti, Mattarei, and Comai are employed by or have received compensation from companies or institutions that received funding from Relmada Therapeutics, Inc. Dr Fava is a consultant to Relmada on behalf of Massachusetts General Hospital and did not receive any personal compensation. Drs Stahl, Pani, Gorodetzky, Vocci, Sapienza, Kosten, Folli, Manfredi, Pappagallo, Kröger, Champasa, Cutler, Maletic, and Inturrisi have received consultant fees from Relmada Therapeutics, Inc. Dr Vocci also is a consultant for Takeda Pharmaceuticals and on the Scientific Advisory Board of Exavir Therapeutics, Inc. Drs O’Gorman and Traversa are employees of Relmada Therapeutics, Inc. Drs De Martin, Mattarei, and Comai have received grant support from MGGM LLC and consultant fees from Neuroarbor LLC, companies affiliated with Relmada Therapeutics. Dr Guidetti has received consultant fees from MGGM LLC. Dr Bushnell is an employee at Cytel, Inc, a company consulting for Relmada. Drs Inturrisi and Manfredi are coinventors of technology related to esmethadone.
Funding/Support: This work was supported by Relmada Therapeutics, Inc, Coral Gables, Florida.
Role of the Sponsor: Relmada Therapeutics participated in the design and conduct of the study; collection, management, analysis, and interpretation of data; and preparation, review, and approval of the manuscript.
Disclaimer: All opinions, conclusions, and data interpretation lie with the authors.
Previous Presentations: American Society of Clinical Psychopharmacology Annual Meeting; June 2023; Miami, Florida; Annual Meeting of the American College of Clinical Pharmacy; November 2023; Dallas, Texas; CNS Summit; November 2023; Boston, Massachusetts; Annual ECNP Congress; October 2023; Barcelona, Spain.
Acknowledgments: Editorial support for the current manuscript was performed by Richard Perry, PharmD, supported by Relmada Therapeutics, Inc, according to Good Publication Practices (GPP3).
ORCID: Paolo L. Manfredi: https://orcid.org/0000-0002-7242-9450
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- The majority of patients fail to achieve remission from first-line antidepressants, and new treatment options are needed. No N-methyl-D-aspartate receptor antagonists are US Food and Drug Administration approved as adjunctive treatment for major depressive disorder.
- This trial of esmethadone did not meet its primary outcome; however, some of the secondary and post hoc outcomes were promising. Esmethadone was overall safe and well tolerated.
References (61)

- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study. Lancet. 2015;386(9995):743–800. PubMed CrossRef
- Hasin DS, Sarvet AL, Meyers JL, et al. Epidemiology of adult DSM-5 Major depressive disorder and its specifiers in the United States. JAMA Psychiatry. 2018;75(4):336–346. PubMed CrossRef
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am. 1996;19(2):179–200. PubMed CrossRef
- Moncrieff J, Cooper RE, Stockmann T, et al. The serotonin theory of depression: a systematic umbrella review of the evidence. Mol Psychiatry. 2023;28:3243–3256. PubMed CrossRef
- Jakobsen JC, Gluud C, Kirsch I. Should antidepressants be used for major depressive disorder? BMJ Evid Based Med. 2020;25:130–136. PubMed CrossRef
- Boku S, Nakagawa S, Toda H, et al. Neural basis of major depressive disorder: beyond monoamine hypothesis. Psychiatry Clin Neurosci. 2018;72(1):3–12. PubMed CrossRef
- Henter ID, de Sousa RT, Zarate CA Jr.. Glutamatergic modulators in depression. Harv Rev Psychiatry. 2018;26:307–319. PubMed CrossRef
- Mathews DC, Henter ID, Zarate CA. Targeting the glutamatergic system to treat major depressive disorder: rationale and progress to date. Drugs. 2012;72:1313–1333. PubMed CrossRef
- Hansen KB, Yi F, Perszyk RE, et al. Structure, function, and allosteric modulation of NMDA receptors. J Gen Physiol. 2018;150:1081–1105. PubMed CrossRef
- Nicoll RA. A brief history of long-term potentiation. Neuron. 2017;93:281–290. PubMed CrossRef
- Autry AE, Adachi M, Nosyreva E, et al. NMDA receptor blockade at rest triggers rapid behavioural antidepressant responses. Nature. 2011;475(7354):91–95. PubMed CrossRef
- Li N, Lee B, Liu RJ, et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science. 2010;329:959–964. PubMed CrossRef
- Cooper T, Seigler MD, Stahl S. Rapid onset brain plasticity at novel pharmacologic targets hypothetically drives innovations for rapid onset antidepressant actions. J Psychopharmacol. 2023;37(3):242–247. PubMed CrossRef
- Correll CU, Solmi M, Cortese S, et al. The future of psychopharmacology: a critical appraisal of ongoing phase 2/3 trials, and of some current trends aiming to de-risk trial programmes of novel agents. World Psychiatry. 2023;22(1):48–74. PubMed CrossRef
- Fogaça MV, Fukumoto K, Franklin T, et al. N-methyl-D-aspartate receptor antagonist d-methadone produces rapid, mTORC1-dependent antidepressant effects. Neuropsychopharmacology. 2019;44:2230–2238. PubMed
- Hanson JE, Yuan H, Perszyk RE, et al. Therapeutic potential of N-methyl-D aspartate receptor modulators in psychiatry. Neuropsychopharmacology. 2024;49(1):51–66. PubMed CrossRef
- Johnston JN, Kadriu B, Kraus C, et al. Ketamine in neuropsychiatric disorders: an update. Neuropsychopharmacology. 2024;49(1):23–40. PubMed CrossRef
- Wang YT, Zhang NN, Liu LJ, et al. Glutamatergic receptor and neuroplasticity in depression: implications for ketamine and rapastinel as the rapid-acting antidepressants. Biochem Biophys Res Commun. 2022;594:46–56. PubMed CrossRef
- Krystal JH, Kavalali ET, Monteggia LM. Ketamine and rapid antidepressant action: new treatments and novel synaptic signaling mechanisms. Neuropsychopharmacology. 2024;49(1):41–50. PubMed CrossRef
- Wilcox MR, Nigam A, Glasgow NG, et al. Inhibition of NMDA receptors through a membrane-to-channel path. Nat Commun. 2022;13(1):4114. PubMed CrossRef
- Bettini E, De Martin S, Mattarei A, et al. The N-methyl-d-aspartate receptor blocker REL-1017 (esmethadone) reduces calcium influx induced by glutamate, quinolinic acid, and gentamicin. Pharmaceuticals (Basel). 2022;15(7):882. PubMed CrossRef
- Bernstein G, Davis K, Mills C, et al. Characterization of the safety and pharmacokinetic profile of D-Methadone, a novel N-Methyl-D-Aspartate receptor antagonist in healthy, opioid-naïve subjects: results of two phase 1 studies. J Clin Psychopharmacol. 2019;39:226–237. PubMed CrossRef
- Fava M, Stahl S, Pani L, et al. REL-1017 (esmethadone) as adjunctive treatment in patients with major depressive disorder: a Phase 2a randomized double-blind trial. Am J Psychiatry. 2022;179(2):122–131. PubMed CrossRef
- Eddy NB, Halbach H, Braenden OJ. Synthetic substances with morphine-like effect: clinical experience; potency, side-effects, addiction liability. Bull World Health Organ. 1957;17:569–863. PubMed
- Gorman AL, Elliott KJ, Inturrisi CE. The d- and l-isomers of methadone bind to the non-competitive site on the N-methyl-D-aspartate (NMDA) receptor in rat forebrain and spinal cord. Neurosci Lett. 1997;223:5–8. PubMed CrossRef
- Pasternak GW, Pan YX. Mu opioids and their receptors: evolution of a concept. Pharmacol Rev. 2013;65:1257–1317. PubMed CrossRef
- Bettini E, Stahl SM, De Martin S, et al. Pharmacological comparative characterization of REL-1017 (esmethadone-HCl) and other NMDAR channel blockers in human heterodimeric N-methyl-d-aspartate receptors. Pharmaceuticals (Basel). 2022;15(8):997. PubMed CrossRef
- Codd EE, Shank RP, Schupsky JJ, et al. Serotonin and norepinephrine uptake inhibiting activity of centrally acting analgesics: structural determinants and role in antinociception. J Pharmacol Exp Ther. 1995;274(3):1263–1270. PubMed
- Fava M, Stahl SM, De Martin S, et al. Esmethadone-HCl (REL-1017): a promising rapid antidepressant. Eur Arch Psychiatry Clin Neurosci. 2023;273:1463–1476. PubMed CrossRef
- Drug Enforcement Administration (DEA). Drug & chemical evaluation section. Drug and chemical information: methadone. Drug and Chemical Information - DEA Diversion Control Division. 2019. https://www.deadiversion.usdoj.gov_chem_info/methadone/methadone.pdf.
- Henningfield J, Gauvin D, Bifari F, et al. REL-1017 (esmethadone; D-methadone) does not cause reinforcing effect, physical dependence, and withdrawal signs in Sprague Dawley rats. Sci Rep. 2022;12(1):11389. PubMed CrossRef
- Levinstein MR, De Oliveira PA, Casajuana-Martin N, et al. Unique pharmacodynamic properties and low abuse liability of the µ-opioid receptor ligand (S)-methadone. Preprint. Posted online December 25, 2023. Mol Psychiatry. doi:10.1038/s41380-023-02353-z. CrossRef
- Olsen GD, Wendel HA, Livermore JD, et al. Clinical effects and pharmacokinetics of racemic methadone and its optical isomers. Clin Pharmacol Ther. 1977;21(2):147–157. PubMed CrossRef
- Shram MJ, Henningfield JE, Apseloff G, et al. The novel uncompetitive NMDA receptor antagonist esmethadone (REL-1017) has no meaningful abuse potential in recreational drug users. Transl Psychiatry. 2023;13(1):192. PubMed CrossRef
- Rickli A, Liakoni E, Hoener MC, et al. Opioid-induced inhibition of the human 5-HT and noradrenaline transporters in vitro: link to clinical reports of serotonin syndrome. Br J Pharmacol. 2018;175:532–543. PubMed CrossRef
- Bonaventura J, Lam S, Carlton M, et al. Pharmacological and behavioral divergence of ketamine enantiomers: implications for abuse liability. Mol Psychiatry. 2021;26(11):6704–6722. PubMed CrossRef
- Stahl SM, De Martin S, Mattarei A, et al. Esmethadone (REL-1017) and other uncompetitive NMDAR channel blockers may improve mood disorders via modulation of synaptic kinase-mediated signaling. Int J Mol Sci. 2022;23(20):12196. PubMed CrossRef
- Bifari F, Pappagallo M, Bleavins M, et al. REL-1017 (Esmethadone), A novel NMDAR blocker for the treatment of MDD is not neurotoxic in Sprague-Dawley rats. Front Pharmacol. 2022;13:863959. PubMed CrossRef
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62. PubMed CrossRef
- Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–389. PubMed CrossRef
- Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266–1277. PubMed CrossRef
- Bremner JD, Krystal JH, Putnam FW, et al. Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J Trauma Stress. 1998;11(1):125–36. PubMed CrossRef
- Ventura J, Lukoff D, Nuechterlein KH, et al. Manual for the expanded brief psychiatric rating scale. Int J Methods Psychiatr Res. 1993;3:227–244.
- Treister R, Trudeau JJ, Van Inwegen R, et al. Development and feasibility of the misuse, abuse, and diversion drug event reporting system (MADDERS®). Am J Addict. 2016;25(8):641–651. PubMed CrossRef
- Rickels K, Garcia-Espana F, Mandos LA, et al. Physician withdrawal checklist (PWC-20). J Clin Psychopharmacol. 2008;28(4):447–451. PubMed CrossRef
- Wesson DR, Ling W. The clinical opiate withdrawal scale (COWS). J Psychoactive Drugs. 2003;35(2):253–259. PubMed CrossRef
- Handelsman L, Cochrane KJ, Aronson MJ, et al. Two new rating scales for opiate withdrawal. Am J Alcohol Abuse. 1987;13:293–308. PubMed CrossRef
- Thase ME, Zhang P, Weiss C, et al. Efficacy and safety of brexpiprazole as adjunctive treatment in major depressive disorder: overview of four short-term studies. Expert Opin Pharmacother. 2019;20(15):1907–1916. PubMed CrossRef
- Daly EJ, Singh JB, Fedgchin M, et al. Efficacy and safety of intranasal esketamine adjunctive to oral antidepressant therapy in treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. 2018;75(2):139–148. PubMed CrossRef
- Popova V, Daly EJ, Trivedi M, et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: a randomized double-blind active-controlled study. Am J Psychiatry. 2019;176(6):428–438. PubMed CrossRef
- Godin O, Leboyer M, Schürhoff F, et al. Metabolic syndrome and illness severity predict relapse at 1-year follow-up in schizophrenia: the FACE-SZ cohort. J Clin Psychiatry. 2018;79(6):17m12007. PubMed CrossRef
- Misdrahi D, Tessier A, Daubigney A, et al. Prevalence of and risk factors for extrapyramidal side effects of antipsychotics: results from the national FACE-SZ cohort. J Clin Psychiatry. 2019;80(1):18m12246. PubMed CrossRef
- Tu TH, Huang KL, Bai YM, et al. Exposure to second-generation antipsychotics and risk of type 2 diabetes mellitus in adolescents and young adults: a nationwide study in Taiwan. J Clin Psychiatry. 2019;80(2):18m12284. PubMed CrossRef
- Molero P, Ramos-Quiroga JA, Martin-Santos R, et al. Antidepressant efficacy and tolerability of ketamine and esketamine: a critical review. CNS Drugs. 2018;32:411–420. PubMed CrossRef
- Ten Have TR, Normand SL, Marcus SM, et al. Intent-to-treat vs. non-intent-to-treat analyses under treatment non-adherence in mental health randomized trials. Psychiatr Ann. 2008;38(12):772–783. PubMed CrossRef
- Tripepi G, Chesnaye NC, Dekker FW, et al. Intention to treat and per protocol analysis in clinical trials. Nephrol Carlt. 2020;25(7):513–517. PubMed CrossRef
- Khan A, Mar KF, Brown WA. Consistently modest antidepressant effects in clinical trials: the role of regulatory requirements. Psychopharmacol Bull. 2021;51(3):79–108. PubMed
- Shiovitz TM, Zarrow ME, Shiovitz AM, et al. Failure rate and “professional subjects” in clinical trials of major depressive disorder. J Clin Psychiatry. 2011;72(9):1284–1285. PubMed CrossRef
- Shiovitz TM, Bain EE, McCann DJ, et al. Mitigating the effects of nonadherence in clinical trials. J Clin Pharmacol. 2016;56(9):1151–1164. PubMed CrossRef
- Freeman MP, Pooley J, Flynn MJ, et al. Guarding the gate: remote structured assessments to enhance enrollment precision in depression trials. J Clin Psychopharmacol. 2017;37(2):176–181. PubMed CrossRef
- Khan A, Schwartz K, Kolts RL, et al. Relationship between depression severity entry criteria and antidepressant clinical trial outcomes. Biol Psychiatry. 2007;62(1):65–71. PubMed CrossRef
This PDF is free for all visitors!





