Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2024;26(2):23f03643
Author affiliations are listed at the end of this article.
Have you ever wondered how you could identify which of your elderly patients is most vulnerable? Have you been concerned about how care can be complicated by the sequelae of trauma? Have you been wary of retraumatizing patients in your effort to manage their distress? Have you been uncertain about whether you could enhance their trust in you and in your recommendations? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Ms X, a 68-year-old woman with a history of coronary artery disease, diabetes mellitus, and cataracts, was admitted to the surgical service with increasingly severe claudication; revascularization was planned. However, while being prepped to go to the operating room, she became panic-stricken and insisted on returning to her room. Shortly after she returned to her room, she left the hospital against medical advice. Two weeks later, with persistent and severe claudication, she was readmitted to the surgical service. Once again, she became filled with panic en route to the operating room, and she insisted upon returning to her room.
A psychiatric consultation was requested. The consultant suspected that Ms X could be a trauma survivor.1 To this end, after establishing rapport with Ms X, the consultant used the Life Events Checklist (LEC)2 to screen Ms X for a history of trauma. The consultant learned that Ms X had been raped as a teenager by a group of men as she walked home from school. She had never told her medical providers about this event. She recounted to the psychiatrist that being hastily undressed in preparation for her surgical procedure brought back the terror and loss of control that she experienced during (and after) her rape. She understood that her surgery was crucial for her ongoing health, and she wanted to undergo the surgery; however, she felt ill equipped to handle the distress that was triggered by her preoperative care.
Following the principles of trauma-informed care (TIC), which emphasize safety, trust, empowerment, choice, and collaboration, the consultant worked with Ms X and her surgical team to develop a collaborative plan that would minimize her psychological distress and allow her to undergo the necessary surgery. The plan included having a nurse review each part of the procedure in detail with Ms X the day before the surgery, allowing her to disrobe herself, and allowing her to maintain control over which of her team members could attend to her needs.
DISCUSSION
What Types of Trauma Experienced Earlier in Life Can Complicate the Lives and Medical Treatments of Elderly Patients?
Traumatic experiences occur throughout the lifespan. Most older adults who experience trauma do not suffer from long-term adverse sequelae. However, for a smaller proportion of older adults, trauma may continue to impede physical and emotional functioning, even when experienced early in life. Impaired functioning caused by trauma may manifest as disorders of affect, behavior, or cognition as well as by medical illnesses, and impaired interpersonal functioning or autonomic arousal.
Myriad traumatic events (eg, natural disasters,3 war,4 interpersonal violence,5 elder mistreatment,6 and surviving the Holocaust7) may increase the risk for psychiatric disorders, impaired functioning, and interpersonal challenges even decades after the initial trauma. Compared to other types of trauma, interpersonal trauma is typically associated with more severe psychopathology.8
Childhood adversity is a type of interpersonal trauma with a documented impact on health and function later in life. Since the original research was published in the 1990s, trauma and chronic instability that occur during childhood and adolescence have been operationalized as adverse childhood experiences (ACEs),9 which are defined as abuse, neglect, and household dysfunction that occurs before the age of 18. Specifically, ACEs include verbal, physical, and sexual abuse, witnessing interpersonal violence between one’s parents, household substance abuse, household mental illness, having incarcerated family members, and parental separation or divorce. ACEs contribute to negative emotional, social, and medical outcomes in later adulthood.9 Importantly, the original research on ACEs showed that the impact of trauma is “dose-dependent,” with the severity of adverse outcomes being dependent upon the type, frequency, and severity of traumatic events.10 The timing of adverse events seems to be important as well, with specific deficits and psychopathology corresponding to certain types of abuse that occur at different developmental stages.11
ACEs have been linked to both psychiatric and medical problems in later life, as well as to interpersonal and affective disturbances. For example, childhood trauma is associated with a higher risk of late-life posttraumatic stress disorder (PTSD),12 depression,13 anxiety,14 personality disorders,15 and substance use disorders.12 Compared to adults with these psychiatric conditions but without a history of ACEs, older adults with ACEs tend to experience symptoms earlier and with a greater severity.16 ACEs have also been linked to a range of medical problems (including arthritis, back problems, high blood pressure, migraine, chronic bronchitis/emphysema/chronic obstructive pulmonary disease [COPD], cancer, stroke, bowel disease, and myalgic encephalomyelitis/chronic fatigue syndrome).17
Underlying these specific psychiatric and medical diagnoses, ACEs are associated with a range of transdiagnostic processes that can interfere with social functioning and cognitive and affective processing18 and lead to increased pain and decreased physical functioning5 as well as hypervigilance, loneliness, aggression, somatization, emotional dysregulation, interpersonal instability, and insecure attachments.19,20 These processes can complicate medical care, interfere with the doctor patient relationship, and elicit strong emotional reactions in clinicians.21
How Can You Identify Which of Your Elderly Patients Are Most Vulnerable?
Trauma may contribute to a range of psychiatric disorders among older adults. In this discussion of assessment, we will focus on PTSD as the disorder with the clearest causal link to trauma. Accurate identification of PTSD in older adults requires an age-appropriate assessment of the diagnostic criteria, as well as an assessment of factors that may place older adults at greater risk for more severe symptomatology.
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5),22 PTSD may only be diagnosed when certain criteria are met. Criterion A defines a traumatic event as exposure to actual or threatened death, serious injury, or sexual violence (through directly experiencing the event, witnessing the event, learning that it occurred, or experiencing repeated exposure to details of the traumatic event). Importantly, not every traumatic event meets this definition. Other types of trauma may contribute to psychopathology but would not warrant assessment or diagnosis of PTSD. The LEC is a useful instrument for determining the nature of the traumatic event. Criterion B describes intrusive symptoms, such as flashbacks or nightmares (1 symptom required). Criterion C addresses persistent avoidance of stimuli associated with the traumatic event(s) (to avoid distressing memories, thoughts, or feelings associated with the traumatic event; 1 symptom required). Criterion D includes impaired cognitions and mood (2 symptoms), and Criterion E specifies changes in arousal and reactivity, including hypervigilance and sleep disturbance (2 symptoms).
The PTSD Checklist for DSM-5 (PCL-5)2 is a commonly used diagnostic tool. The commonly used PCL-5 threshold for likely PTSD is 33, although some researchers recommend a lower threshold for older adults, given lower overall symptom endorsement among this population.23
When evaluating older adults, it is helpful to remember that symptoms of PTSD may manifest in different ways. Compared with younger adults, older adults with PTSD report less severe symptoms, fewer intrusive thoughts, and less avoidance, while endorsing higher levels of hypervigilance and more somatic symptoms.24 Subthreshold PTSD is far more common than full PTSD, and it is also associated with impaired psychological functioning. Thus, even in the absence of full DSM-5 PTSD criteria, patients may still experience distressing and impairing traumatic reactions.25 Early-life trauma is associated with an increased risk for a range of psychiatric illnesses among older adults; thus, a trauma history should be assessed independently of any specific diagnosis. Importantly, care must be taken when inquiring about painful traumatic events, such as childhood maltreatment or sexual abuse, as older patients may be reluctant to disclose this information.26
Numerous factors increase an older adult’s vulnerability to trauma-related pathology. Demographic factors (such as lesbian, gay, bisexual, transgender, queer [LGBTQ+] identity,27 female sex,28 and black race/ethnicity29) all increase the risk for psychopathology following trauma. Life stressors may also be relevant; PTSD can manifest as a fluctuating course among older adults or may be dormant until it is reactivated by a new stressor or a trauma that arises in later life.30 Therefore, older adults with a trauma history who are experiencing significant stress in the form of illness, loss, life transition, or functional impairment may be vulnerable to increased symptom severity.
Personal and interpersonal variables are also relevant to trauma-related pathology. For example, personality features, such as high neuroticism and low extraversion, have been shown to mediate the relationship between childhood trauma and late-life depression and anxiety.31 Trauma increases the risk for disrupted attachment in older adults, putting them at risk for loneliness, impaired coping with stressful situations, and poor social support.19 Older adults who felt invalidated by others following their traumatic experiences may also be at increased risk for problems in later life,32 as may those who have experienced racial or ethnic discrimination.33 Importantly, for providers, older adults who were victimized as children are at greater risk of being revictimized in later life.34 This underscores the importance of assessing older patients for current physical, sexual, and emotional abuse, neglect, and financial fraud.35
Awareness of older patients’ demographic risk factors and experiences with discrimination and invalidation, and assessment of patients’ loneliness, social support, and coping skills can help clinicians identify patients who most need trauma-informed approaches. This information may also help providers protect their patients against future revictimization.
How Common Are Physical, Sexual, and Emotional Abuse and Neglect in Adulthood?
Although much attention has been paid to understanding the various types of abuse (eg, physical, sexual, or emotional) and neglect in childhood, they are also common in adults. Physical abuse among adults encompasses the intentional use of force that results in harm or injury, and it can be inflicted by intimate partners, family members, or staff in institutional settings. According to the National Intimate Partner and Sexual Violence Survey (NISVS),36 nearly 20 people every minute are physically abused by an intimate partner in the United States; this accounts for more than 10 million adults (both women and men) who experience such abuse each year. Moreover, approximately 1 in 4 women and 1 in 7 men have been the victim of severe violence (eg, beatings, burnings, or strangulation) at the hands of an intimate partner. Among the elderly, physical abuse is an important public health problem. A large systematic review (involving 52 geographically diverse studies)37 reported that adults older than 60 have experienced physical abuse in community or institutional settings at rates ranging from 2.6% to 14.1%, respectively. Emerging data also indicate that the prevalence rates of any form of abuse, including physical abuse, in both community and institutional settings substantially increased during the COVID-19 pandemic; thus, approaches to TIC should be tailored specifically to the geriatric population.38
Sexual abuse refers to nonconsensual sexual activity that is imposed upon an individual, regardless of their gender. Certain groups face a higher risk of sexual abuse, including those who have been subjected to coercive behaviors in intimate partner relationships, members of vulnerable populations (eg, sex workers, individuals with physical or functional disabilities, and those with serious mental illness or cognitive impairment), individuals in institutional settings (eg, nursing homes and residential care facilities), and those who are marginalized or socioeconomically disadvantaged (eg, individuals facing poverty, racial discrimination, homelessness, and low social support).39 Extensive research that spans more than 40 years suggests that sexual abuse is common in adulthood. It is estimated that approximately 17%–25% of women and 1%–3% of men have been sexually abused during their lifetime; moreover, according to the NISVS, approximately 1 in 5 women and 1 in 71 men in the United States have been raped.36,40,41 Nevertheless, sexual abuse is commonly underreported, and these survey rates may be an underestimate of the true extent of the problem.
Emotional or psychological abuse often occurs in adult relationships with intimate partners, family members, friends, and colleagues. Certain individuals are at a higher risk of experiencing emotional abuse, including those who have been subjected to psychological manipulation in intimate partner relationships, the elderly residing in institutional care settings, and individuals with intellectual disabilities.42 The lifetime prevalence rate for emotional abuse varies by gender, with women consistently reporting higher rates of emotional abuse over their lifespan compared to men.43
Neglect of adults can manifest in a variety of contexts (eg, caregiving relationships, dependent adult relationships, and situations where individuals fail to adequately care for themselves). However, there is a scarcity of epidemiologic data regarding the prevalence of neglect in adulthood. The paucity of research in this area underscores the need for further investigation to understand the drivers and the impact of adult neglect. By bridging these knowledge gaps, clinicians can develop more effective strategies for prevention and intervention in cases of adult neglect in myriad settings. These efforts will contribute to enhancing their well being and safety.
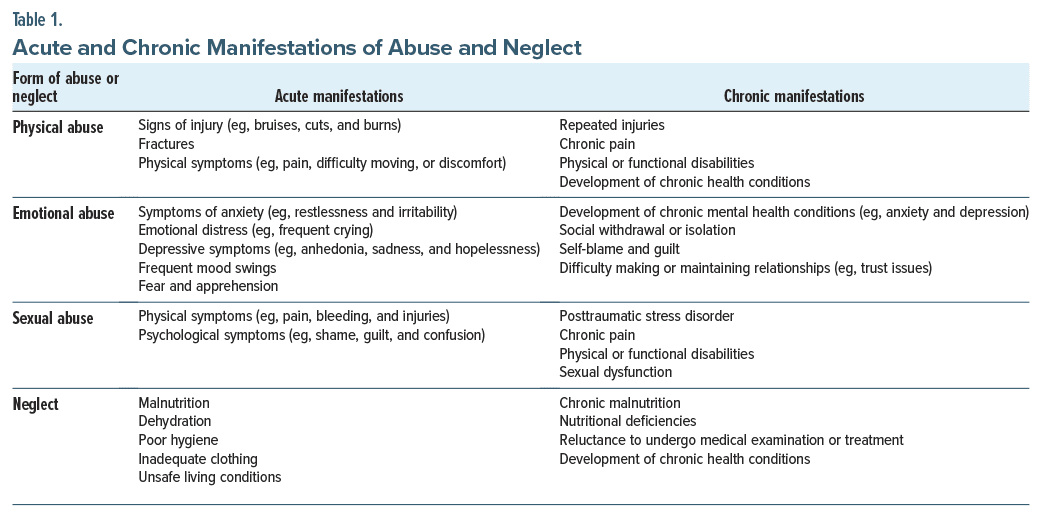
What Are the Acute and Chronic Manifestations and Sequelae of Abuse and Neglect?
Table 1 lists several acute and chronic manifestations of abuse and neglect. In brief, the signs and symptoms that arise in response to maltreatment include physical injuries, emotional distress, fear, and neglect-related health issues. Chronic manifestations often involve profound and enduring effects on physical and mental health (eg, chronic pain, psychiatric disorders, difficulties forming and maintaining social relationships, and chronic health problems).
What Is Meant by TIC and Who Can Provide It?
TIC is based upon the principles and practices of understanding and responding to the high prevalence and widespread impact of trauma.44 The 4 “Rs” of TIC are realizing the impact of trauma in the general population, recognizing its signs and symptoms, responding by integrating knowledge of the impact of trauma across all levels of the institution, and making all efforts to avoid retraumatizing survivors.45 The key components of TIC are assuring safety, trustworthiness, and transparency; providing peer support; being collaborative; facilitating empowerment; and providing care in a cultural and historical context with sensitivity to gender issues.45 Anyone who cares for patients (on an individual, organizational, or policy level) is encouraged to embrace the principles of TIC.
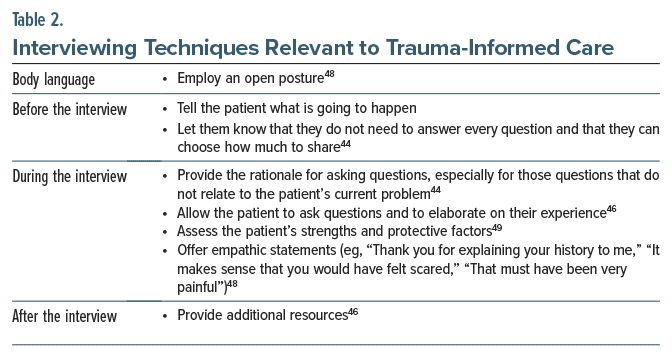
Several TIC concerns are relevant to the care of older adults. Given the high prevalence of abuse and neglect, all patients should be screened for a trauma history. Interviewers should be mindful of general cultural, historical, and gender issues for their patients while inquiring about their individual experience.46 Older adults may not perceive their life events as traumatic and view labeling their experiences as such as being self indulgent. As a result, they may minimize or deny their experiences.47 Given the inherent power imbalance between interviewers and patients, interviewers should emphasize that they are working on a team, and the patient’s strengths (eg, resilience and support systems) should be highlighted.46 Finally, interviews should adapt to the clinical context and the role of the interviewer (Table 2).44,46,48,49
How Can You Enhance Trust in You and in Your Recommendations?
Opportunities for enhancing trust in your recommendations include prioritizing clear communication and transparency around clinical decision-making, enhancing clinical continuity by offering provider consistency and thorough chart review, acknowledging that your patient may have had retraumatizing interactions with health care providers, and demonstrating a commitment to avoid repetition of those mistakes.
Clear communication. Trustworthiness and transparency form the foundation of health care. Ashworth and colleagues46 recently recommended that providers introduce themselves and their role in their patient’s care at the beginning of each visit and then state their goals for the appointment; in addition, they suggested that clinicians explicitly ask their patients whether they have any questions for them. Before any procedures, even noninvasive ones, the rationale for the procedure should be reviewed (and include how the information gleaned from the examination or test will be used to further their care).46 When planning treatment, each option should be discussed in layperson’s terms; this facilitates asking the patient about their hopes and concerns related to each path, leaving time for questions, whenever possible.50 Although the next steps of treatment may appear obvious to health care providers, these steps may not be clear for patients.
Continuity. Patients with a history of trauma often endorse frustration around a lack of continuity in their health care providers, as this lack of continuity inhibits the development of trust in their health care team,51 and feeling that providers may not understand their history or its context.51 Unfortunately, provider continuity is not always feasible. However, trust can be enhanced by demonstrating that you have thoroughly reviewed your patient’s medical record before their visit and that you will take the time to listen carefully to their story.
Efforts to prevent retraumatization. Trust can also be facilitated by avoiding retraumatization. Organizations and health care systems can inadvertently create situations and environments that are reminiscent of your patient’s trauma (by creating a sense of disempowerment and helplessness).52 It is also useful to avoid unintentional blaming of the victim, which quickly erodes trust. Such an approach is particularly important when your patient feels marginalized and discriminated against (due to their race, gender identity, sexual orientation, disability, or another stigmatized status).53
How Can the Sequelae of Trauma Be Managed?
The sequelae of trauma can be managed through psychotherapy, medications, or a combination of both. The American Psychological Association (APA) strongly recommends the use of cognitive-behavioral therapy (CBT), cognitive therapy, cognitive processing therapy (CPT), and prolonged exposure (PE) therapy for individuals with PTSD.54
CBT is a widely used form of therapy that helps patients to identify and modify unhelpful or harmful thoughts and beliefs, thereby resulting in positive changes to thoughts, feelings, and behaviors.55 Cognitive therapy focuses primarily on thoughts or cognitions. In CPT, patients are taught to identify “stuck points” and challenge trauma-related beliefs that adversely impact their functioning.56 Finally, in PE therapy, patients engage in imaginal exposures of the traumatic event, and in vivo exposures to associated feared stimuli.57 Treatments with a provisional recommendation by the APA include eye movement desensitization and reprocessing (EMDR), narrative exposure therapy (NET), and brief eclectic therapy.54
In addition to these cognitive behavioral and exposure based interventions, other psychotherapies that can help manage the sequelae of trauma are life review therapy, spiritually focused therapy, and integrative treatments.23,58 Yoga and mindfulness-based interventions are effective and feasible options that can be adjunctive or an alternative to traditional talk therapies.59,60 While there is a dearth of literature on evidence-based interventions for older adults with PTSD, there is a larger body of research that supports evidence-based interventions for older adults with depression. In general, older adults are likely to benefit from mental health treatment.23
It is useful to know that older adults engaging in psychotherapy may have age-related health concerns, such as impairments in cognition, hearing, and vision, as well as pain.23 Apprehension about cardiovascular or respiratory issues can be addressed through careful monitoring and collaboration with a patient’s physician. Most older adults can tolerate exposure-based therapies that may induce a stress response.61 Attention should be given to other psychiatric comorbidities, and a TIC approach should be used throughout.23
The primary pharmacologic treatments for PTSD and trauma-related sequelae (eg, anxiety and depression) are the selective serotonin reuptake inhibitors (SSRIs), such as sertraline, fluoxetine, escitalopram, and paroxetine, and the serotonin-norepinephrine reuptake inhibitors (SNRIs), such as venlafaxine.62 Additional medications include mirtazapine, a noradrenergic and specific serotonergic antidepressant, and amitriptyline, a tricyclic antidepressant. Providers should exercise caution when prescribing psychotropics to older adults and consider the risks and benefits in the context of a patient’s current treatment plan and medical morbidities.63 For example, benzodiazepines and beta-blockers may lead to adverse health effects (eg, increasing the risks for falls) among older adults.64 Escitalopram and sertraline have also been recommended over other SSRIs because they have fewer drug-drug interactions.65 Providers can refer to clinical guidelines and best practices for prescribing medications for older adults, such as the Beers Criteria.66
How Can Emotional Reactions to Past Trauma Interfere With Medical Examinations and Treatments?
Medical examinations or procedures may serve as triggers for traumatic memories that pose challenges to communication, patient-provider trust, medical examinations, and treatments. Patients with a history of trauma may experience heightened anxiety and fear when faced with medical settings, examinations, or treatments. These distressful feelings can interfere with their ability to provide accurate medical information, discuss their concerns with their provider, and follow treatment recommendations, particularly when managing multiple medications and their potential interactions. The interference in communication brought on by these feelings of distress may further result in skepticism or resistance to recommended medical interventions and hinder accurate treatment planning. Beyond communication complications, some patients with a trauma history may engage in avoidance behavior to protect themselves from reexperiencing distressing emotions or memories. While patients may engage in avoidance as a protective behavior, avoidance may contribute to resistance to undergoing necessary medical examinations or treatments, effectively reducing the patient’s ability to access necessary care. As a result, patients may miss appointments, fail to follow prescribed medications, or disengage from recommended therapies due to emotional barriers. Additionally, trauma can influence an individual’s perception of pain, potentially leading to heightened pain sensitivity and emotional numbing in response to pain. Either response may influence pain reporting, complicate the management of pain and other conditions, and cloud treatment decisions.67,68 Further, trauma-related stress can manifest in physical symptoms that have no apparent medical cause, leading to various unexplained physical complaints, posing additional challenges for health care providers in differentiating between trauma-related symptoms and other medical issues.
Patients who have experienced trauma may exhibit angry outbursts, negative mood states, difficulty trusting authority figures, and wariness about medical advice, all of which may create problematic interactions with medical providers.69–71 At its worst, difficulties in or strain on the patient-provider relationship may lead to misdiagnosed symptoms. For example, nightmares and emotional or behavioral outbursts may be mistaken for symptoms of other conditions like Alzheimer’s disease, rather than being related to the patient’s history of trauma.72,73 More commonly, when reactions due to past trauma are poorly understood, this misinterpretation may lead to patients being viewed negatively and labeled as “difficult” and interfere with the quality of care received.74
A myriad of reactions to past trauma can interfere with medical examinations and treatments. Patients with a history of repeated injuries may develop chronic pain, physical disabilities, and chronic health conditions that can hinder their ability to undergo medical examinations and treatments effectively. Chronic manifestations of anxiety, depression, and social withdrawal can lead to reluctance in seeking or complying with medical care. For example, individuals who have experienced sexual trauma may suffer from PTSD and sexual dysfunction, which may effect their willingness to undergo sensitive medical examinations. Additionally, adults who have endured neglect may exhibit reluctance to undergo medical examination due to the long-standing effects of neglect, such as a history of malnutrition, dehydration, or living in unsafe conditions. In these ways, a patient’s history of trauma may influence their feelings or perceptions of medical settings as safe spaces in which they can trust providers to perform examinations with care and recommend necessary treatments in earnest. Understanding and addressing these reactions empathically is essential for providing effective care in medical settings that may be seen as safe and ensuring the well-being of those who have experienced trauma.
How Often Do Traumatic Experiences Arise in the Elderly and Get Reactivated by Therapeutic Interventions?
Most adults older than 65 have experienced some form of trauma during their lifetime; the lifetime prevalence among this age group is as high as 70%.75 Unfortunately, many events that are experienced as we age can reactivate memories of trauma that in turn may interfere with adherence to treatment and medical examinations. The frequency with which reactivation occurs due to medical examinations and treatments is influenced by the nature of the trauma experienced, the type of medical treatment, and the characteristics of individual patients and providers. Exposure to a similar environment within which the trauma was experienced increases the likelihood of reactivation. For example, for some patients preparing for surgical treatment may trigger unwanted memories and feelings related to past traumas. The severity and recency of the traumatic experience may effect the intensity of memory reactivation in these circumstance. Experiences of severe traumas may have a more profound and lasting impact on patients’ responses, and the more recent the traumatic event, the more likely it may be to resurface during medical procedures.23 Additionally, whether the individual has had adequate time and support in coping with their trauma may affect the likelihood of memory reactivation. Importantly, as traumatic experiences and their effects can accumulate throughout life, older adults may be particularly susceptible to the reactivation of traumatic memories.
Reactivated memories often retain a vivid intensity and a feeling of present threat, even when reactivation occurs decades after the original trauma.23,76 These memories can be reactivated by common age-related events, such as changes in health status and mobility, the loss of social support networks following retirement, or the deaths of loved ones.23,77 Additionally, some evidence suggests that older adults may respond with stress-related symptoms more often than younger adults, particularly when experiencing events like the loss of a spouse,78 the risk of which increases with age.23
Older adults are more likely to have experienced certain types of trauma that can affect the risk of reactivation during medical examinations. Since it is more likely for older adults to have faced major medical events, surgeries, and health challenges without the benefit of contemporary medical advancements and technology, these medical experiences can influence their experience and perception of care in the present.79 Older adults are more likely to have experienced multiple personal losses, as well as historical events (such as World War II, the Korean War, and the Vietnam War) that may have involved direct exposure to violence, loss, and displacement.80 Adults from racial and ethnic minority groups may have also experienced historical racial discrimination, segregation, or civil rights struggles, which have lasting psychological, social, and physical health impacts and contribute to disparate health outcomes. While older adults may have experienced these potentially traumatic events, each generation may have unique traumas and stressors, and understanding these differences is crucial for providing age-appropriate TIC and support.
By recognizing and addressing the potential for trauma reactivation, health care providers can contribute to the overall well-being of their patients and ensure that respectful medical care can be delivered in a manner that considers their emotional needs. In this way, health care professionals can create a supportive and understanding environment that reduces the risk of trauma-related distress during medical procedures. The implementation of TIC practices during medical procedures can minimize the chances of reactivating traumatic memories. Being sensitive to trauma history, creating a safe environment, and providing appropriate support can mitigate the potential for reactivation. Understanding the factors that contribute to trauma in this population and tailoring therapeutic interventions is crucial to promoting their well-being and safety.23
What Are the Behavioral and Medical Sequelae of Trauma?
Traumatic experiences can influence health-related choices and behaviors, interactions with medical providers, and health care utilization. Past trauma can create barriers to seeking health care, including the fear of medical settings, distrust of health care providers, or difficulty expressing health concerns due to trauma related symptoms. Trauma survivors may struggle with adhering to medical treatment plans, which can affect their ability to manage chronic conditions and achieve better health outcomes. Some forms of trauma can alter an individual’s perception of their health, leading to a focus on physical symptoms and perceived vulnerabilities rather than overall well-being. Traumatic experiences can effect an individual’s self-efficacy in health behaviors, leading to reduced self-care and neglect of health needs. Further, trauma survivors may engage in risky behaviors or have a sense of invulnerability, which can lead to increased exposure to health risks.81
Other medical comorbidities can interact with the sequelae of trauma-related symptoms bi-directionally to further compromise overall health. For example, PTSD frequently co-occurs with chronic conditions like COPD. PTSD symptoms may worsen adherence to COPD treatment, and COPD exacerbations may, in turn, interact with and worsen PTSD symptoms.82 Further, among those living with PTSD, there is an increased risk for accelerated aging and disability. Importantly, these effects of comorbidities can be particularly pronounced in end-of life care settings, where patients may struggle to describe their traumatic experiences, and symptoms may be misinterpreted as other conditions.75 Additionally, the emotional distress caused by trauma can lead to an increase in appetitive behaviors, such as eating, drinking, and smoking. In this way, traumatic experiences can lead to negative health behaviors and negatively effect quality of life, leading to lower reported levels of well-being and life satisfaction.83 Some studies suggest that individuals with high ACEs scores may experience accelerated biological aging, which can manifest in cellular and molecular changes.84,85 Individuals with a history of ACEs may utilize health care services more frequently due to an increased risk of physical and mental health issues.86,87 Further, adults who experienced ACEs may also engage in unhealthy coping mechanisms or adopt poor health behaviors,88 such as smoking, excessive alcohol consumption, sedentary lifestyles, and poor dietary habits. These coping behaviors may increase trauma survivors’ risk of developing chronic health conditions, such as cardiovascular disease, autoimmune disorders, gastrointestinal disorders, and chronic pain syndromes. The physiological impact of trauma itself may further contribute to the development or exacerbation of these conditions.
Sensory changes associated with aging can be influenced by trauma. Hearing loss, which is common among older adults, can lead to mishearing and an increased risk of auditory hallucinations (associated with PTSD). Adjusting communication methods (such as using hearing aids, pocket talkers, and adjusting voice tone, speed, and volume) may be necessary in facilitating effective communication. Trauma can also affect the amount of pain that patients report, and it is essential to encourage reporting and educate patients, rather than accepting the notion that pain is a normal part of aging.75
Overall, the influence of trauma on current health behaviors is multifaceted, affecting cognitive functioning, sensory perception, pain perception, and psychiatric conditions. Understanding these influences and adopting strategies that consider the specific needs of patients with trauma histories is crucial for providing effective and empathetic care.
THE SIGNIFICANT IMPACT OF PAST TRAUMA ON HEALTH BEHAVIORS TODAY
Reactions to past trauma can vary widely, from disengagement to tearful recounting to panic, leading to problematic interactions with medical providers. Patients may exhibit resistant behavior or experience reactivating memories during medical examinations, influencing their willingness to seek or comply with medical care. The role of comorbidities is also crucial, with trauma-linked PTSD being associated with increased risk for chronic health conditions and accelerated aging. Cognitive, sensory, and pain-related alterations may also be observed in patients with trauma histories. Understanding these effects and adopting strategies to address patients’ unique needs is essential for providing effective and empathic care in medical settings. Understanding the impact of trauma on health behaviors is essential in order for health care providers and support systems to provide TIC. Tailoring interventions that address the emotional and psychological aspects of trauma can help create a supportive environment that encourages healthier behaviors and promotes overall well-being for trauma survivors. By recognizing the potential influence of trauma on health behaviors, health care providers can offer appropriate support and interventions to address trauma-related challenges and promote positive health outcomes.
What Are the Benefits of Facing Past Traumas in the Present?
Being the beneficiary of support and treatment for past traumas can be dramatically helpful (eg, reducing the adverse effects on physical and mental health [such as depression, PTSD, problematic substance use and loneliness, obesity, and inflammatory bowel diseases]).18,89,90 For example, in a study of middle-aged and older adults, investigators identified that individuals with more feelings of mastery over their lives demonstrated greater resilience against the adverse health effects of trauma.44 Treating trauma-related illness can provide patients with insight on the connection between prior experiences and current medical and psychological disorders. This insight offers opportunities for trauma-exposed patients to address the role that trauma has played in their lives, increasing their agency to make helpful health decisions and foster mastery over their lives. For older adults, unaddressed sequelae of trauma exposure (eg, depression, hypertension, obesity, diabetes, excessive alcohol consumption, and low social contact) become risk factors for cognitive decline.91 Fortunately, each of these conditions is modifiable, and those who address them may be able to mitigate the multiple risk factors for poor cognitive health later in life. Thus, from a medical perspective, addressing and treating trauma can have preventive benefits that help reduce patients’ risk for adverse health outcomes.
What Happened to Ms X?
After undergoing a successful operation, Ms X was discharged from the hospital to complete her recovery at home. As part of her discharge instructions, she received information about mental health services in her area. A few weeks later, she began treatment with a mental health counselor in her community who helped her to better understand how traumatic experiences early in life can lead to enduring symptoms of anxiety, depression, or posttraumatic stress across the lifespan. Ms X engaged in a 12-week, evidence-based trauma treatment that alleviated many of her trauma-related mental health symptoms.
CONCLUSION
Traumatic experiences occur throughout the lifespan; unfortunately, even when they were experienced early in life, they may continue to impede physical and emotional functioning. Moreover, the impact of childhood trauma is “dose-dependent,” with the severity of adverse outcomes being dependent upon the type, frequency, and severity of traumatic events.
Patients with a history of trauma may experience heightened anxiety and fear when faced with medical settings, examinations, or treatments; these distressing feelings can interfere with patients’ ability to provide accurate medical information, discuss their concerns with their provider, and follow treatment recommendations. When the principles of TIC are used to guide providers’ behavior, patients are more likely to feel safe, empowered, and respected and are thus more likely to collaboratively engage in their care.
In instances where trauma-related disorders contribute to clinical distress and/or functional impairments in older adults, a range of psychotherapeutic and psychopharmacologic treatments have demonstrated efficacy in managing these conditions.
Article Information
Published Online: April 23, 2024. https://doi.org/10.4088/PCC.23f03643
© 2024 Physicians Postgraduate Press, Inc.
Submitted: September 14, 2023; accepted December 18, 2023.
To Cite: Popescu D, Mellen E, Ander I, et al. Caring for traumatized elders: lessons learned from trauma-informed care. Prim Care Companion CNS Disord. 2024;26(2): 23f03643.
Author Affiliations: Department of Psychiatry, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts (all authors).
Author Information: Drs Popescu, Vyas, Ishikawa, Mellen, and Ander are co-first authors.
Corresponding Author: Rachel Zack Ishikawa, PhD, MPH, Department of Psychiatry, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114 ([email protected]).
Relevant Financial Relationships: Dr Vyas has received research support from Nestlé Purina PetCare Company, Mars Edge, and American Foundation for Suicide Prevention. All other authors report no conflicts of interest related to the subject of this article.
Funding/Support: None.
Clinical Points
- Patients with a history of trauma may experience heightened anxiety and fear when faced with medical settings, examinations, or treatments; these distressful feelings can interfere with their ability to provide accurate medical information, discuss their concerns with their provider, and follow treatment recommendations, particularly when managing multiple medications and their potential interactions, and may result in skepticism or resistance to recommended medical interventions.
- The 4 “Rs” of trauma-informed care are realizing the impact of trauma in the general population, recognizing its signs and symptoms, responding by integrating knowledge of the impact of trauma across all levels of the institution, and making all efforts to avoid retraumatizing survivors.
- Opportunities for enhancing trust in your recommendations include prioritizing clear communication and transparency around clinical decision making, enhancing clinical continuity by offering provider consistency and thorough chart review, acknowledging that your patient may have had retraumatizing interactions with health care providers, and demonstrating a commitment to avoid repetition of those mistakes.
References (91)

- Goodman LA, Sullivan CM, Serrata J, et al. Development and validation of the trauma-informed practice scales. J Community Psychol. 2016;44(6):747–764. CrossRef
- Weathers FW, Blake DD, Schnurr PP, et al. Life Events Checklist for DSM-5 (LEC-5). PTSD: National Center for PTSD; 2013. Accessed June 29, 2023. https://www.ptsd.va.gov/professional/assessment/documents/LEC5_Standard_Self-report.PDF
- Cherry KE, De Vito AN, Calamia MR, et al. Disaster stressors and psychological well-being in older adults after a flood. Psychol Aging. 2021;36(5):660–666. PubMed CrossRef
- Ron P. Posttraumatic stress disorder among three-generation families in times of war: a comparison between Israeli Jewish and Arabs after the Second Lebanon War (2006) and Cast Lead Operation (2009). Traumatology. 2014;20(4):269–276. CrossRef
- Walser RD, Oser ML, Tran CT, et al. Frequency and impact of trauma in older women: a military and nonmilitary sample. J Loss Trauma. 2016;21(1):62–73. CrossRef
- Cisler JM, Amstadter AB, Begle AM, Hernandez M, Acierno R, et al. Elder mistreatment and physical health among older adults: the South Carolina Elder Mistreatment Study. J Trauma Stress. 2010;23(4):461–467. PubMed CrossRef
- Kimron LG, Marai I, Lorber A, et al. The long-term effects of early-life trauma on psychological, physical and physiological health among the elderly: the study of Holocaust survivors. Aging Ment Health. 2019;23(10):1340–1349. PubMed CrossRef
- Bachem R, Levin Y, Solomon Z. Trajectories of attachment in older age: interpersonal trauma and its consequences. Attach Hum Dev. 2019;21(4):352–371. PubMed CrossRef
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245–258. PubMed CrossRef
- Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356–e366. PubMed CrossRef
- Teicher MH, Parigger A. The “Maltreatment and Abuse Chronology of Exposure” (MACE) scale for the retrospective assessment of abuse and neglect during development. PLoS One. 2015;10(2):e0117423. PubMed CrossRef
- Rhee TG, Barry LC, Kuchel GA, et al. Associations of adverse childhood experiences with past-year DSM-5 psychiatric and substance use disorders in older adults. J Am Geriatr Soc. 2019;67(10):2085–2093. PubMed CrossRef
- Ege MA, Messias E, Thapa PB, et al. Adverse childhood experiences and geriatric depression: results from the 2010 BRFSS. Am J Geriatr Psychiatry. 2015;23(1):110–114. PubMed CrossRef
- Van Assche L, Van de Ven L, Vandenbulcke M, et al. Ghosts from the past? The association between childhood interpersonal trauma, attachment and anxiety and depression in late life. Aging Ment Health. 2020;24(6):898–905. PubMed CrossRef
- Raposo SM, Mackenzie CS, Henriksen CA, et al. Time does not heal all wounds: older adults who experienced childhood adversities have higher odds of mood, anxiety, and personality disorders. Am J Geriatr Psychiatry. 2014;22(11):1241–1250. PubMed CrossRef
- Hovens JGFM, Giltay EJ, Wiersma JE, et al. Impact of childhood life events and trauma on the course of depressive and anxiety disorders. Acta Psychiatr Scand. 2012;126(3):198–207. PubMed CrossRef
- Afifi TO, MacMillan HL, Boyle M, et al. Child abuse and physical health in adulthood. Health Rep. 2016;27(3):10–18. PubMed
- Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on neurobiological, psychosocial, and somatic conditions across the lifespan. Front Psychiatry. 2018;9:420. PubMed CrossRef
- Peters M. Trauma and attachment in older patients with common mental disorders. GeroPsych: J Gerontopsychol Geriatr Psychiatry. 2023;36(1):11–21. CrossRef
- Su WM, Stone L. Adult survivors of childhood trauma: complex trauma, complex needs. Aust J Gen Pract. 2020;49(7):423–430. PubMed CrossRef
- Dalenberg CJ. Maintaining the safe and effective therapeutic relationship in the context of distrust and anger: countertransference and complex trauma. Psychother Theory Res Pract Train. 2004;41(4):438–447. CrossRef
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
- Pless Kaiser A, Cook JM, Glick DM, et al. Posttraumatic stress disorder in older adults: a conceptual review. Clin Gerontol. 2019;42(4):359–376. PubMed CrossRef
- Rutherford BR, Zilcha-Mano S, Chrisanthopolous M, et al. Symptom profiles and treatment status of older adults with chronic post-traumatic stress disorder. Int J Geriatr Psychiatry. 2021;36(8):1216–1222. PubMed CrossRef
- Çayır E, Burke MP, Spencer M, et al. Lifetime trauma and depressive symptomatology among older American Indians: the Native Elder Care Study. Community Ment Health J. 2018;54(6):740–747. PubMed
- McInnis-Dittrich K. Adapting life-review therapy for elderly female survivors of childhood sexual abuse. Fam Soc. 1996;77(3):166–173. CrossRef
- Camacho D, Rodriguez CV, Moore KL, et al. Older immigrant Latino gay men and childhood sexual abuse: findings from the Palabras Fuertes project. Qual Soc Work. 2022;21(5):932–955. PubMed CrossRef
- Lamoureux-Lamarche C, Vasiliadis HM. Lifetime traumatic events, health-related quality of life, and satisfaction with life in older adults. Qual Life Res. 2017;26(10):2683–2692. PubMed CrossRef
- McLaughlin KA, Alvarez K, Fillbrunn M, et al. Racial/ethnic variation in trauma related psychopathology in the United States: a population-based study. Psychol Med. 2019;49(13):2215–2226. PubMed CrossRef
- Chopra MP, Zhang H, Pless Kaiser A, et al. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am J Geriatr Psychiatry. 2014;22(1):86–97. PubMed CrossRef
- Gomes Jardim GB, von Gunten A, da Silva Filho IG, et al. Relationship between childhood maltreatment and geriatric depression: the mediator effect of personality traits. Int Psychogeriatr. 2019;31(12):1759–1767. PubMed CrossRef
- Eising CM, Voelkle MC, Rohner SL, et al. Lifetime post-traumatic stress disorder in older individuals with a history of institutional upbringing in childhood: the role of social acknowledgement and stressful life events. Eur J Psychotraumatol. 2021;12(1):1915578. PubMed CrossRef
- Olson MD. The influence of social exclusion on posttraumatic stress reactions in older adult veterans. Soc Work. 2020;65(2):123–130. PubMed CrossRef
- Kong J, Easton SD. Re-experiencing violence across the life course: histories of childhood maltreatment and elder abuse victimization. J Gerontol B Psychol Sci Soc Sci. 2019;74(5):853–857. PubMed CrossRef
- Singh BK, Rustad JK, McWilliams G, et al. Financial abuse of older adults: screening, prevention, and interventions by primary care providers. Prim Care Companion CNS Disord. 2023;25(3):22f03434. PubMed CrossRef
- Black MC, Basile KC, Breiding MJ, et al. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2011.
- Yon Y, Mikton CR, Gassoumis ZD, et al. Elder abuse prevalence in community settings: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(2):e147–e156. PubMed CrossRef
- Chang ES, Levy BR. High prevalence of elder abuse during the COVID-19 pandemic: risk and resilience factors. Am J Geriatr Psychiatry. 2021;29(11):1152–1159. PubMed CrossRef
- Tharp AT, DeGue S, Valle LA, et al. A systematic qualitative review of risk and protective factors for sexual violence perpetration. Trauma Violence Abuse. 2013;14(2):133–167. PubMed CrossRef
- Sutherland S, Scherl DJ. Patterns of response among victims of rape. Am J Orthopsychiatry. 1970;40(3):503–511. PubMed CrossRef
- Tjaden P, Thoennes N. Prevalence and consequences of male-to-female and female-to-male intimate partner violence as measured by the National Violence Against Women Survey. Violence Against Women. 2000;6(2):142–161. CrossRef
- Karakurt G, Silver KE. Emotional abuse in intimate relationships: the role of gender and age. Violence Vict. 2013;28(5):804–821. PubMed CrossRef
- Chiu GR, Lutfey KE, Litman HJ, et al. Prevalence and overlap of childhood and adult physical, sexual, and emotional abuse: a descriptive analysis of results from the Boston Area Community Health (BACH) survey. Violence Vict. 2013;28(3):381–402. PubMed CrossRef
- Elliot AJ, Turiano NA, Infurna FJ, et al. Lifetime trauma, perceived control, and all cause mortality: results from the Midlife in the United States Study. Health Psychol. 2018;37(3):262–270. PubMed CrossRef
- SAMHSA. Concept of Trauma and Guidance for a Trauma-Informed Approach. Substance Abuse & Mental Health Services Administration; 2014.
- Ashworth H, Lewis-O’Connor A, Grossman S, et al. Trauma-informed care (TIC) best practices for improving patient care in the emergency department. Int J Emerg Med. 2023;16(1):38. PubMed CrossRef
- Hiskey S, McPherson S. That’s just life: older adult constructs of trauma. Aging Ment Health. 2013;17(6):689–696. PubMed CrossRef
- Brown T, Mehta PK, Berman S, et al. A trauma-informed approach to the medical history: teaching trauma-informed communication skills to first-year medical and dental students. MedEdPORTAL. 2021;17:11160. PubMed CrossRef
- Roberts SJ, Chandler GE, Kalmakis K. A model for trauma-informed primary care. J Am Assoc Nurse Pract. 2019;31(2):139–144. PubMed CrossRef
- Grossman S, Cooper Z, Buxton H, et al. Trauma-informed care: recognizing and resisting re-traumatization in health care. Trauma Surg Acute Care Open. 2021;6(1):e000815. PubMed CrossRef
- Matthew A, Moffitt C, Huth-Bocks A, et al. Establishing trauma-informed primary care: qualitative guidance from patients and staff in an urban healthcare clinic. Children (Basel). 2022;9(5):616. PubMed CrossRef
- SAMHSA (Substance Abuse and Mental Health Services Administration). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach (HHS Publication No. SMA 14-4884). Substance Abuse and Mental Health Services Administration; 2014. Accessed July 5, 2023. https://store.samhsa.gov/system/files/sma14-4884.pdf
- Seedat S. Commentary on the special issue on disproportionate exposure to trauma: trauma, stress, and adversities and health disparities among disenfranchised groups globally during the COVID pandemic. J Trauma Stress. 2021;34(5):1061–1067. PubMed CrossRef
- American Psychological Association. Summary of Recommendations of the APA Guideline Development Panel for the Treatment of PTSD. American Psychological Association; 2017.
- Arch JJ, Craske MG. First-line treatment: a critical appraisal of cognitive behavioral therapy developments and alternatives. Psychiatr Clin North Am. 2009;32(3):525–547. PubMed CrossRef
- Resick PA, Monson CM, Chard KM. Cognitive Processing Therapy Veteran/Military Version: Therapist’s Manual. PsycEXTRA Dataset. American Psychological Association; 2008.
- Foa EB, Hembree EA, Cahill SP, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics. J Consult Clin Psychol. 2005;73(5):953–964. PubMed CrossRef
- Ishikawa RZ, Ander I, Popescu DL, et al. Child maltreatment among older adults: a narrative review of psychotherapeutic interventions and clinical considerations. Clin Gerontol. 2023. EPub ahead of print:1–15. 10.1080/07317115.2023.2219671 CrossRef
- Hazlett-Stevens H, Singer J, Chong A. Mindfulness-based stress reduction and mindfulness-based cognitive therapy with older adults: a qualitative review of randomized controlled outcome research. Clin Gerontol. 2019;42(4):347–358. PubMed CrossRef
- Martens NL. Yoga interventions involving older adults: integrative review. J Gerontol Nurs. 2022;48(2):43–52. CrossRef
- Cook JM, McCarthy E, Thorp SR. Older adults with PTSD: brief state of research and evidence-based psychotherapy case illustration. Am J Geriatr Psychiatry. 2017;25(5):522–530. PubMed CrossRef
- Management of Posttraumatic Stress Disorder and Acute Stress Disorder Work Group. VA/DOD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder: clinician summary. Focus (Am Psychiatr Publ). 2018;16(4):430–448. PubMed CrossRef
- Leahy LG. Caution is key when prescribing for older adults. J Psychosoc Nurs Ment Health Serv. 2017;55(12):7–10. PubMed CrossRef
- Crocco EA, Jaramillo S, Cruz-Ortiz C, et al. Pharmacological management of anxiety disorders in the elderly. Curr Treat Options Psychiatry. 2017;4(1):33–46. PubMed CrossRef
- Lenze EJ, Ajam Oughli H. Antidepressant treatment for late-life depression: considering risks and benefits. J Am Geriatr Soc. 2019;67(8):1555–1556. PubMed CrossRef
- The 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052–2081. PubMed
- Asmundson GJG, Katz J. Understanding pain and posttraumatic stress disorder comorbidity: do pathological responses to trauma alter the perception of pain? Pain. 2008;138(2):247–249. PubMed CrossRef
- Sherman AL, Morris MC, Bruehl S, et al. Heightened temporal summation of pain in patients with functional gastrointestinal disorders and history of trauma. Ann Behav Med. 2015;49(6):785–792. PubMed CrossRef
- Block SD. Psychological issues in end-of-life care. J Palliat Med. 2006;9(3):751–772. PubMed CrossRef
- Feldman DB. Posttraumatic stress disorder at the end of life: extant research and proposed psychosocial treatment approach. Palliat Support Care. 2011;9(4):407–418. PubMed CrossRef
- Feldman DB, Periyakoil VS. Posttraumatic stress disorder at the end of life. J Palliat Med. 2006;9(1):213–218. PubMed CrossRef
- Mevissen L, Lievegoed R, de Jongh A. EMDR treatment in people with mild ID and PTSD: 4 cases. Psychiatr Q. 2011;82(1):43–57. PubMed CrossRef
- Mevissen L, Lievegoed R, Seubert A, et al. Treatment of PTSD in people with severe intellectual disabilities: a case series. Dev Neurorehabil. 2012;15(3):223–232. PubMed CrossRef
- Glick DM, Cook JM, Moye J, et al. Assessment and treatment considerations for post traumatic stress disorder at end of life. Am J Hosp Palliat Care. 2018;35(8):1133–1139. PubMed CrossRef
- Ganzel BL. Trauma-informed hospice and palliative care. Gerontologist. 2018;58(3):409–419. PubMed CrossRef
- Hiskey S, Luckie M, Davies S, et al. The phenomenology of reactivated trauma memories in older adults: a preliminary study. Aging Ment Health. 2008;12(4):494–498. PubMed CrossRef
- Wilcox S, Evenson KR, Aragaki A, et al. The effects of widowhood on physical and mental health, health behaviors, and health outcomes: The Women’s Health Initiative. Health Psychology. 2003;22(5):513–522. PubMed CrossRef
- Asher S, Starr R. Time doesn’t heal all wounds: incorporating trauma-informed principles in practice. J Gerontol Nurs. 2021;47(10):54–56. PubMed CrossRef
- Hansen MC, Ghafoori B, Diaz M. Examining attitudes towards mental health treatment and experiences with trauma: understanding needs of trauma exposed middle aged and older adults. J Community Psychol. 2020;48(5):1452–1468. PubMed CrossRef
- Wilmoth JM, Landes SD, London AS, et al. The health of male veterans in later life. Innov Aging. 2019;3(suppl 1):S214. CrossRef
- Kantor V, Knefel M, Lueger-Schuster B. Perceived barriers and facilitators of mental health service utilization in adult trauma survivors: a systematic review. Clin Psychol Rev. 2017;52:52–68. PubMed CrossRef
- Teixeira PJZ, Porto L, Kristensen CH, et al. Post-traumatic stress symptoms and exacerbations in COPD patients. COPD. 2015;12(1):90–95. PubMed CrossRef
- Bellis MA, Hardcastle K, Ford K, et al. Does continuous trusted adult support in childhood impart life-course resilience against adverse childhood experiences – a retrospective study on adult health-harming behaviours and mental well-being. BMC Psychiatry. 2017;17(1):110. PubMed CrossRef
- Danese A, Moffitt TE, Harrington H, et al. Adverse childhood experiences and adult risk factors for age-related disease: depression, inflammation, and clustering of metabolic risk markers. Arch Pediatr Adolesc Med. 2009;163(12):1135–1143. PubMed CrossRef
- Shalev I, Entringer S, Wadhwa PD, et al. Stress and telomere biology: a lifespan perspective. Psychoneuroendocrinology. 2013;38(9):1835–1842. PubMed CrossRef
- Dong M, Giles WH, Felitti VJ, et al. Insights into causal pathways for ischemic heart disease: adverse childhood experiences study. Circulation. 2004;110(13):1761–1766. PubMed CrossRef
- Lown EA, Phillips F, Schwartz LA, et al. Psychosocial follow-up in survivorship as a standard of care in pediatric oncology. Pediatr Blood Cancer. 2015;62(suppl 5):S514–S584. PubMed CrossRef
- Kelly-Irving M, Lepage B, Dedieu D, et al. Adverse childhood experiences and premature all-cause mortality. Eur J Epidemiol. 2013;28(9):721–734. PubMed CrossRef
- Fink DS, Galea S. Life course epidemiology of trauma and related psychopathology in civilian populations. Curr Psychiatry Rep. 2015;17(5):31. PubMed CrossRef
- Monnat SM, Chandler RF. Long term physical health consequences of adverse childhood experiences. Sociol Q. 2015;56(4):723–752. PubMed CrossRef
- Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!



