Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2024;26(6):24f03768
Author affiliations are listed at the end of this article.
Have you been faced with the challenge of managing a patient with comorbid bipolar disorder and posttraumatic stress disorder (PTSD)? Have you been uncertain whether impulsivity, sleeplessness, and problematic relationships were due to one disorder or the other? Have you been concerned that the management of one disorder would interfere with the treatment of the other? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Ms C, a 46-year-old woman with a psychiatric history of major depressive disorder (MDD), attention deficit/hyperactivity disorder, PTSD, heavy alcohol use, and obesity, was referred by her therapist for the evaluation and management of worsening mood symptoms. She had a long history of fluctuating moods with periodic hypomania (ie, with increased energy, elevated mood, increased goal-directed activity, talkativeness, and impulsive/excessive spending) that could last up to 2 months and occur several times each year. She described herself as an extrovert; however, when she became depressed, she became isolated and had low mood, anhedonia, low energy levels, sleep disturbances, and hopelessness and functioned poorly. Her depressive episodes ranged from moderate to severe; however, she had never engaged in self harming behaviors. Her son was thought to have bipolar disorder.
She endorsed symptoms of PTSD that followed multiple traumatic events in her youth. She described having nightmares (of being killed) that led to insomnia and staying awake all night (once every few months, although the PTSD symptoms had improved compared to the past). She was receiving trauma focused cognitive-behavioral therapy (CBT). In addition, she had panic attacks for which she received lorazepam on a nightly basis; other medications included citalopram (20 mg daily) and amphetamine dextroamphetamine (5 mg twice daily), which might have contributed to a more unstable mood. She endorsed a history of heavy alcohol use; however, currently, she drank 3 drinks on weekends. Based on her mood symptoms, her mood disorder diagnosis was revised to bipolar disorder with rapid-cycling features.
DISCUSSION
How Often Do Bipolar Disorder and PTSD Coexist?
Studies examining PTSD in those with bipolar disorder have estimated rates as high as 40% for inpatient1 and community samples2 (with a lifetime prevalence of 16%),3 which is double that of PTSD in the general population.
What Are the Shared Risk Factors for Bipolar Disorder and PTSD?
Despite the high prevalence of PTSD in those with bipolar disorder, the etiology of comorbid bipolar disorder and PTSD remains incompletely understood. Notably, there is significant overlap in risk factors for both PTSD and bipolar disorder, including exposure to trauma(s), co-occurrence of other psychiatric illnesses, a lack of social support, a lower socioeconomic status, and personality factors (such as high neuroticism and low extraversion, at least while in the depressed phase of bipolar disorder).3 In addition, trauma is reported frequently by those with bipolar disorder (preceding the onset of the disease), with some estimates reported to be as high as one-third in individuals with bipolar disorder.4 Finally, illness-associated symptoms of bipolar disorder, including risk-taking and impulsivity, may place patients at risk for trauma, especially while manic, with trauma exposure rates as high as 98%.1,5,6
Which Symptoms of Bipolar Disorder and PTSD Overlap?
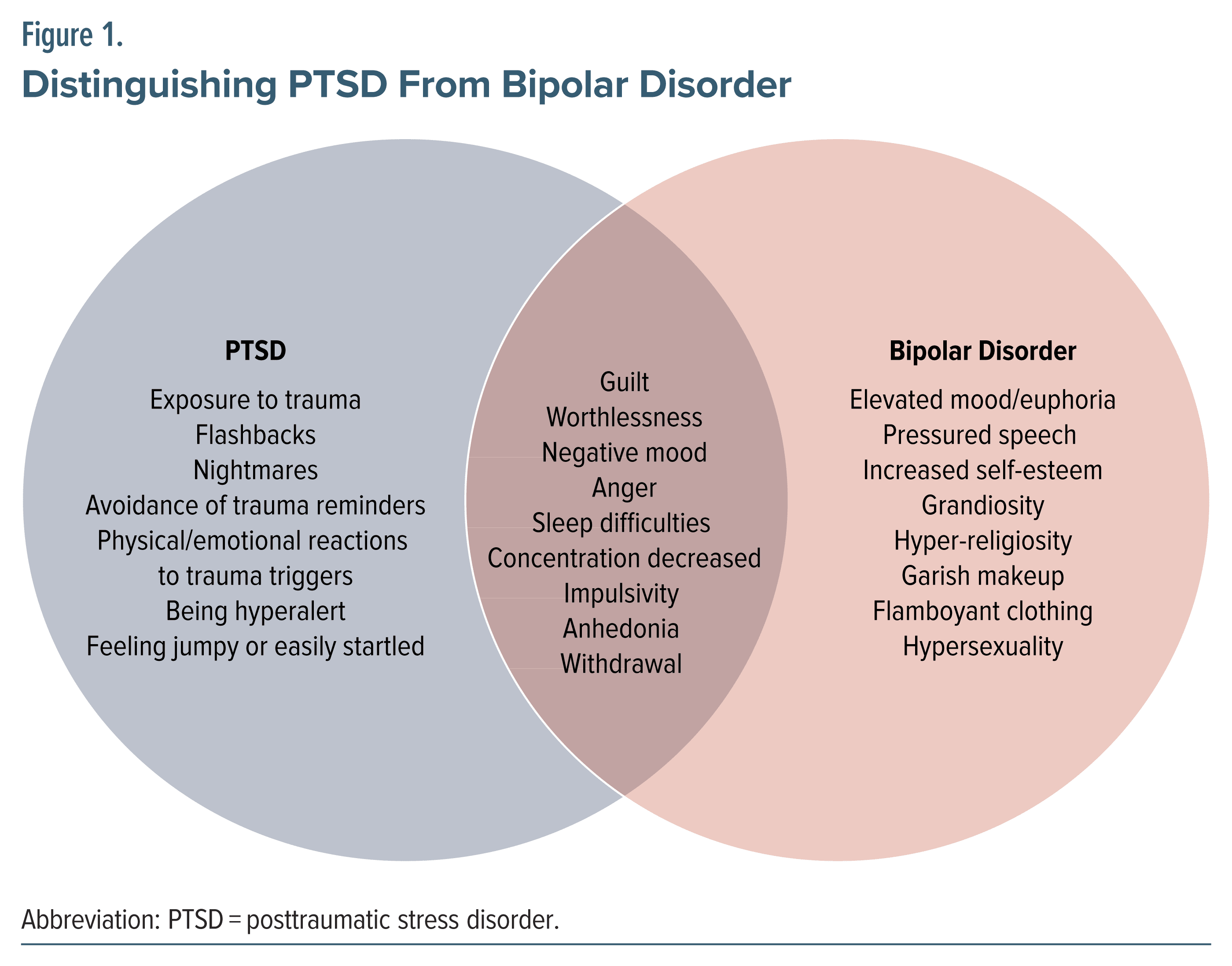
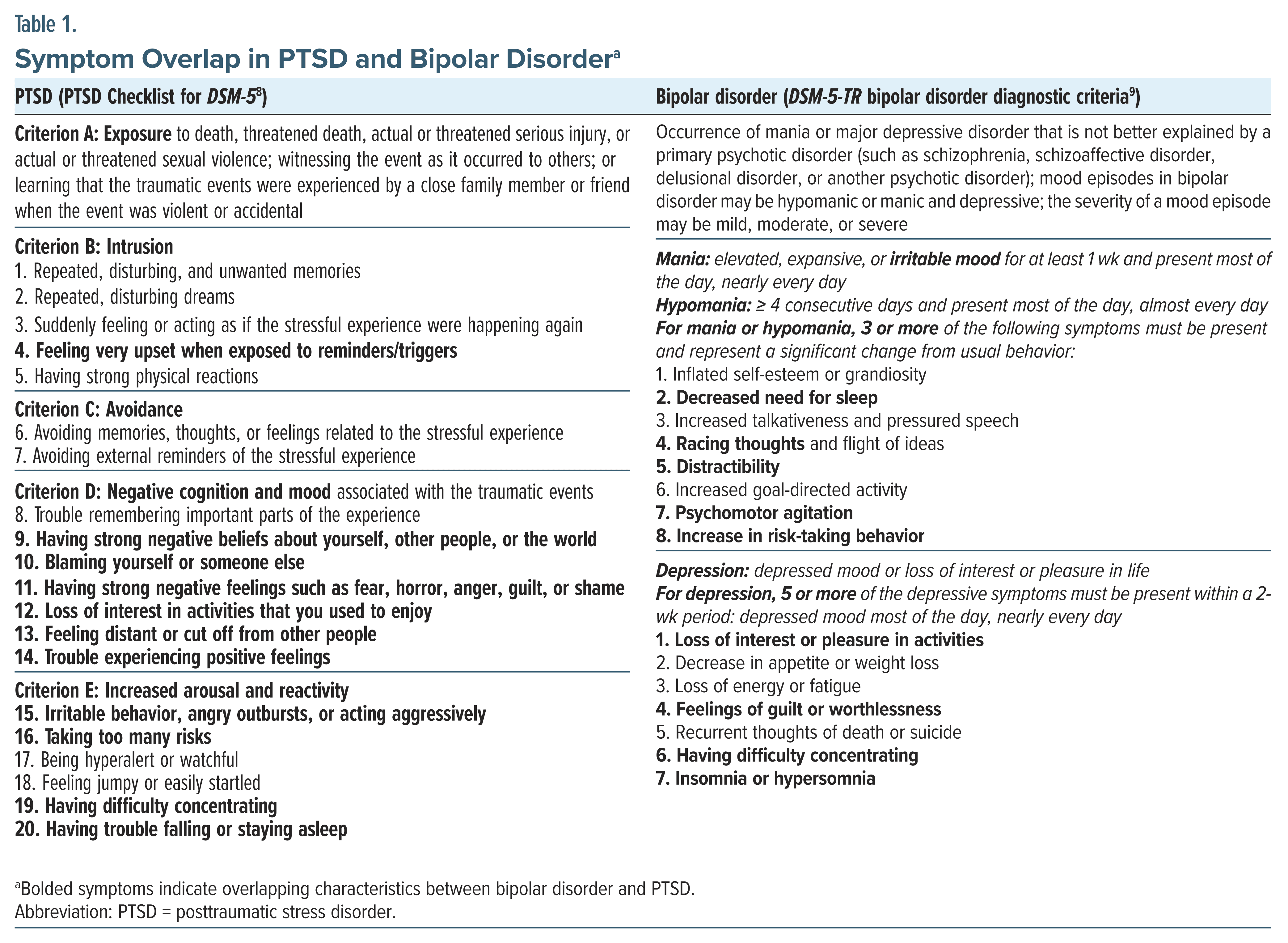
Although many manifestations of bipolar disorder and PTSD overlap (Figure 1), several characteristics help to clarify the diagnosis. Exposure to traumatic events is a key factor in the development of PTSD (criterion A): direct exposure to actual or threatened death, serious injury, or sexual violence; witnessing the event as it occurred to others; or learning that the traumatic events were experienced by a close family member or friend when the event was violent or accidental.7 The traumatic event may lead to reexperiencing symptoms (eg, intrusive memories, nightmares, flashbacks, and hyperarousal), avoidance, and negative alterations in cognition and mood that were associated with the traumatic events.7 In contrast, bipolar disorder is characterized by mood episodes (including depression, hypomania, or mania). Unlike PTSD, the mood symptoms of bipolar disorder are not necessarily triggered by traumatic events. The criteria (and their overlap) for PTSD and bipolar disorder are highlighted in Table 1.8,9
How Can Clinicians Determine Whether Symptomatic Exacerbations Are Due to Bipolar Disorder or PTSD?
Following trauma, symptoms associated with trauma related stress often arise and can lead to the development of an acute stress disorder (ASD) and PTSD; the onset and duration of symptoms distinguish between the 2 disorders. ASD can be diagnosed after 3 days and up to 1 month following traumatic stress, while PTSD cannot be diagnosed until 1 month has passed.7 Individuals with PTSD are more likely to meet diagnostic criteria for at least one other mental disorder (including MDD, bipolar disorder, generalized anxiety disorder, or an alcohol use disorder or substance use disorder [SUD]) than those without PTSD.10,11
Distinguishing between a trauma-related stress disorder and bipolar disorder requires detailed knowledge of the history, which includes considering triggers that are linked to trauma exposure in PTSD, and DSM-5 diagnostic criteria. In addition, the episodic nature of symptoms and mood episodes associated with bipolar disorder plays a crucial role in making an accurate diagnosis. The use of rating scales can facilitate making a diagnosis of bipolar disorder; the Young Mania Rating Scale is one of the most frequently used tools to assess manic symptoms, whereas the Patient Health Questionnaire-9 is commonly used to screen for depressive symptoms,12,13 while the PTSD Checklist for DSM-5 provides a self-report of PTSD symptoms8 (Table 1). Anxious ruminations are often mistaken for racing thoughts (and vice versa). Although individuals with PTSD may experience racing thoughts and pressured speech, speech in bipolar disorder may be unrelenting, rapid, excited, and without pauses, with a flight of ideas (where thoughts jump from one idea to another) and loose associations (describing an unclear or unrelated idea) that are difficult to interrupt. Speech in bipolar disorder may also have a sing-song quality, with clang phenomena (pairing words with a similar sound). Bipolar disorder may manifest through inappropriate laughter, extreme cheerfulness, humor, and singing. Individuals with mania are often hypersexual and may offer spontaneous sexual content. Thought content in mania usually includes hyper-religiosity and delusions of grandeur (eg, about their special powers, abilities, or fame). They may present themselves as overly confident and cheerful, with an expansive affect (eg, extremely elevated mood accompanied by high energy levels). In bipolar disorder, insomnia often involves a decreased need for sleep (eg, going for days with little to no sleep, yet not feeling tired). Other symptoms suggestive of bipolar disorder include euphoria, increased self-esteem, and grandiosity.
With intrusive symptoms, those with PTSD may become upset when exposed to reminders of their trauma. While individuals with PTSD often connect their distress to trauma triggers, a straightforward connection between symptoms and the triggering event often goes unnoticed. Differentiating flashbacks in PTSD from hallucinations that may occur in psychotic disorders (eg, schizophrenia, schizoaffective disorder, mania, and MDD with psychotic features, as well as in delirium, alcohol withdrawal delirium tremens, or other substance intoxication- or withdrawal-induced disorders) is crucial. Flashbacks in PTSD often stand out by their direct connection to trauma and their occurrence in the absence of psychotic, medical, or substance-induced disorders.
With criterion D, a bevy of negative cognitive and mood symptoms in PTSD overlap with the signs and symptoms of bipolar disorder. There may be a tendency to blame oneself, others, or the world. Overlapping symptoms in PTSD and bipolar disorder include a negative or low mood, feelings of guilt or worthlessness, loss of interest, anger, or fear. Anhedonia (an inability to feel pleasure from things that used to bring joy or happiness) is common in both conditions. Individuals may have difficulty experiencing positive emotions in both PTSD and the depressive phase of bipolar disorder. Trauma related hyperarousal and reactivity (criterion E) include symptoms that overlap with bipolar disorder, including irritability, anger, aggression, and risk taking behaviors. The ability to concentrate may be impaired in both PTSD and bipolar disorder. While insomnia may occur in both, trauma-related nightmares are common in PTSD. Prazosin is often prescribed to help with PTSD-related nightmares (starting at 1 mg at bedtime and increasing to 3–20 mg at bedtime); for additional prescribing guidance, see the VA/DoD Clinical Practice Guideline 2023.7
How Can PTSD and Its Treatments Complicate Bipolar Disorder Management?
According to a review of the literature by Cerimele and colleagues14 of individuals with bipolar disorder, women with bipolar disorder and those with bipolar I disorder experience a higher prevalence of PTSD. Individuals with bipolar disorder and PTSD have a high symptom burden and a low quality of life.14 Using the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) dataset (N = 3,158), Hernandez and colleagues15 evaluated differences in the prevalence of PTSD between those with bipolar I and II disorder. Their findings indicated that more participants with bipolar I disorder were diagnosed with co-occurring PTSD, but there was no significant difference in reexperiencing, avoidance, or arousal symptoms of PTSD between subgroups of those with bipolar I or II disorder.15
Having a history of childhood trauma(s) can have a lasting impact on the development and progression of bipolar disorder. It can lead to an earlier onset of bipolar disorder, more lifetime depressive episodes, more severe symptoms during both manic and depressive episodes, and a longer duration of untreated bipolar disorder.16,17 Moreover, the presence of PTSD in patients with bipolar disorder has been associated with an accelerated course of illness, a lower age at onset of manic/hypomanic episodes, a younger age at the time of diagnosis of bipolar disorder, earlier initiation of illicit drug use, more lifetime manic and hypomanic episodes, and greater functional impairment than those with only bipolar disorder.18 The comorbidity of bipolar disorder and PTSD tends to adversely impact the course and prognosis of each disorder, including an increased risk of rapid mood cycling, poor quality of life, and a higher risk of suicide compared with those with either disorder alone.19,20
The Clinical and Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder study (Bipolar CHOICE) recruited 482 individuals with bipolar disorder and compared the pharmacologic efficacy of medication trials. Utilizing these study data, Katz and colleagues21 conducted a hierarchical multiple regression analysis to assess whether comorbid PTSD was associated with more thoughts of suicide in bipolar disorder in a cross-sectional study design. The authors21 used the Concise Health Risk Tracking Scale total and factor scores while controlling for common correlates of suicidal ideation (eg, a current major depressive episode, a comorbid anxiety disorder, illness severity, and prior suicide attempts). The authors21 noted that all participants with comorbid bipolar disorder and PTSD (N = 58) were more likely to have made a suicide attempt (P < .001) and have current thoughts of suicide (P = .005) compared to those without PTSD.
Bipolar disorder and SUDs commonly coexist.22 Moreover, patients diagnosed with bipolar disorder have a 61% lifetime prevalence of SUD.23 Others have examined the prevalence and nature of co-occurring disorders among treatment-seeking patients diagnosed with current bipolar disorder and an SUD.24 Of 90 participants diagnosed with bipolar I (n = 75, 78%) or II disorder, nearly one-fourth (22%) and almost one-half (48%), respectively, had a lifetime anxiety disorder, with PTSD being the most common co-occurring disorder (23%). The study24 suggested that those with comorbid PTSD, but not other anxiety disorders, began using drugs at an earlier age and had more lifetime SUDs, particularly cocaine and amphetamine use disorders, than those without PTSD. Further examination revealed that most of the participants with PTSD were women, that sexual abuse was the most frequently reported index trauma, and that the mean age of the earliest index trauma occurred before the mean age of initiation of drug use.24 The authors24 emphasized the importance of investigating the ramifications of a trauma history among those who had both bipolar disorder and SUD.
Other investigators25 have found that individuals with bipolar disorder and PTSD were less likely to be in recovery (ie, with relative euthymia) at STEP-BD study entry and to have a lower role attainment and quality of life than those with bipolar disorder without PTSD. Patients with comorbid bipolar disorder and PTSD were more likely to suffer from mood episodes during an 8-week follow-up period compared to those without PTSD. Greater depressive symptom burden and psychosocial impairment have been found in those with bipolar disorder and PTSD despite guideline-concordant care for patients with bipolar disorder during the STEP-BD study.26 In addition, those with comorbid bipolar disorder and PTSD had significantly higher mean Clinical Global Impressions–Severity scores and required more frequent inpatient psychiatric treatment.27 Patients with bipolar disorder and PTSD and those with only bipolar disorder were less likely to have received psychotherapy and antidepressant pharmacotherapy than those with PTSD.27
A recent systematic review28 that examined the impact of PTSD on pharmacologic interventions in adults with bipolar disorder found that comorbid PTSD may affect the response to quetiapine and lithium in those with bipolar disorder. The investigators28 noted higher response rates with lithium in those with bipolar disorder alone compared with those with comorbid bipolar disorder and PTSD over a 4-year observational study period. In addition, more severe symptoms were reported in the bipolar disorder–PTSD group compared to those with bipolar disorder alone following 6 months of quetiapine treatment in a randomized, controlled study. However, the authors28 suggested that these results should be viewed as preliminary due to a high risk of bias and a low quality of evidence. In terms of PTSD treatment, the use of antidepressants (which are first line treatments for PTSD) should be used with caution in those with comorbid bipolar disorder, given the increased risk of inducing rapid cycling, mixed states, and manic episodes.3,29
How Can Bipolar Disorder Treatment Complicate PTSD Management?
Treatment of bipolar disorder in the context of PTSD adds complexity to the management of PTSD, primarily due to the potential interactions between these 2 conditions and the side effects of medications used for their treatment. For example, lithium, a mood-stabilizing agent that is effective in preventing mood recurrences, can cause cognitive impairment.30 In those with comorbid PTSD, who may already experience cognitive difficulties, lithium can potentiate existing symptoms and adversely impact daily functioning. In addition, antiepileptic drugs, such as valproate and carbamazepine, are also mood stabilizers used to treat bipolar disorder; however, at higher doses, they have been associated with hepatic dysfunction, which requires careful monitoring and dose adjustment to mitigate the risk of hepatotoxicity. Furthermore, while benzodiazepines are not a first-line treatment for bipolar disorder, they can swiftly alleviate acute manic symptoms, such as agitation and insomnia, especially early in the illness before the effects of mood stabilizers emerge.31 Unfortunately, these medications can provoke disinhibition and paradoxical reactions, such as impulsivity, reckless behavior, and poor judgment.32 These risks are especially concerning in those with comorbid bipolar disorder and PTSD, who frequently manifest heightened arousal, hypervigilance, and impulsivity.33 Benzodiazepines can also exacerbate these symptoms and elevate the risk of disinhibition. If cognitive impairment, emotional dysregulation, substance use, and psychosocial stressors arise, treatment nonadherence may follow. Moreover, avoidance and hypervigilance that are commonplace in PTSD may interfere with treatment engagement for bipolar disorder, further complicating the management of both disorders.
Fortunately, nonpharmacologic strategies, including lifestyle and behavioral modifications, have been promising in the management of bipolar disorder34; however, individuals with comorbid PTSD often have a heightened startle response and hypervigilance, which can make engaging in lifestyle changes, such as tension reducing physical exercise, challenging. In addition, stress reduction techniques, such as mindfulness and relaxation exercises, often alleviate manic symptoms in bipolar disorder.35 However, individuals with PTSD may have a heightened sensitivity to stress and may become distressed when engaging in relaxation exercises or mindfulness practices.36 For those with bipolar disorder and PTSD, relaxation techniques may inadvertently trigger trauma-related memories or increase anxiety and agitation. While maintaining social connections and engaging in supportive relationships facilitates emotional well-being in those with bipolar disorder,37 individuals with PTSD may manifest social withdrawal or have difficulty trusting others due to past traumas. Encouraging social engagement may have adverse effects on those with bipolar disorder and PTSD, potentially triggering vulnerability, anxiety, and hypervigilance.
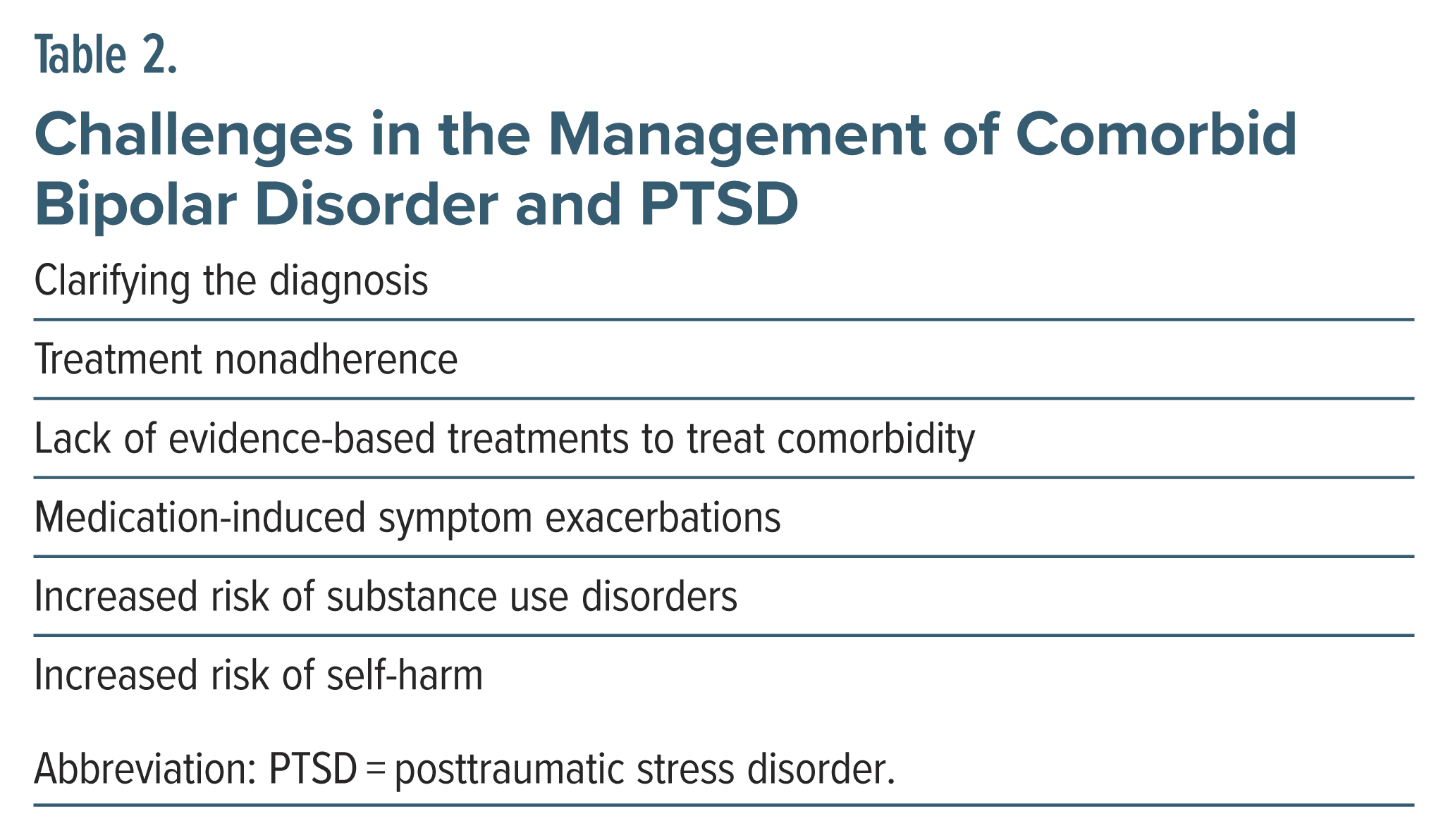
In summary, clinicians should be prepared for the challenges faced by individuals with bipolar disorder and PTSD and tailor treatments to address both conditions concurrently while minimizing the risk of exacerbating symptoms of PTSD. A multi-disciplinary collaborative care approach that involves mental health professionals with expertise in treating both bipolar disorder and PTSD is key for optimizing outcomes and enhancing the overall quality of life for individuals with these psychiatric comorbidities. Table 2 highlights the main challenges that clinicians face when treating comorbid bipolar disorder and PTSD.
Which Medications Are Safe and Efficacious for Patients With Bipolar Disorder and PTSD?
Although the literature indicates that PTSD is highly comorbid with bipolar disorder, studies of the effectiveness of pharmacologic interventions in both conditions are lacking.14 The medications used in the treatment of bipolar disorder and PTSD include mood stabilizers, atypical antipsychotics, antidepressants, and benzodiazepines.3 However, in patients with coexisting bipolar disorder and PTSD, mood stabilizers are often recommended as the first-line treatment to address symptoms of bipolar disorder, followed by pharmacotherapy for PTSD, once the maintenance phase of bipolar disorder has been achieved.
According to an observational study,38 the use of lithium was associated with a higher response rate in bipolar disorder alone compared with use in comorbid bipolar disorder and PTSD over a period of 4 years. Another study39 assessed the mean scores on the Bipolar Inventory of Symptom Scale (BISS) at baseline and at the end of 24-week treatment follow-up; they found that at baseline, patients with comorbid bipolar disorder and PTSD had greater symptom severity compared to those with bipolar disorder alone. However, no significant differences were observed at follow-up between the 2 groups while receiving lithium.39 Results from a 12- week double-blind, placebo-controlled trial involving 15 subjects (including those with both civilian- and military-related traumas) showed that lamotrigine could be effective in the treatment of PTSD.40 More patients receiving lamotrigine responded (50%) than those who received a placebo (25%). Patients who received lamotrigine had less reexperiencing, avoidance, and numbing symptoms compared to those in the placebo group.40
Results of open trials have suggested that valproate might be effective for PTSD. However, data from controlled studies are lacking. For instance, in an open clinical trial, 16 Vietnam veterans with PTSD were treated with valproate, and 10 of them had fewer arousal and avoidance symptoms, but the treatment did not reduce their intrusive symptoms.41 Carbamazepine has also been efficacious for bipolar disorder, although the findings in anxiety disorders are less conclusive. Nevertheless, uncontrolled open-label trials have shown that carbamazepine has been associated with a reduction in intrusive traumatic memories and flashbacks, as well as beneficial effects in insomnia, irritability, impulsivity, and violent behavior.42,43 A retrospective case series examining topiramate in those with bipolar disorder and comorbid conditions suggested symptomatic improvement in comorbid bipolar disorder and PTSD.44 Moreover, oxcarbazepine may have reduced symptoms of PTSD in a patient with comorbid bipolar disorder and PTSD after 4 weeks of treatment with persistence of effects for over 16 months.45
A review of the efficacy of atypical antipsychotics in 12 prospective, controlled studies that used validated rating scales of PTSD symptoms46 found that atypical antipsychotics were both safe and effective, although there were some negative outcomes. Atypical antipsychotics were also effective in treating anxiety, depression, and psychotic symptoms that are frequently associated with PTSD.46 Olanzapine was more effective in reducing overall PTSD symptoms than placebo or fluphenazine in 3 out of 4 studies. On the other hand, in 4 out of 7 studies, risperidone was superior to placebo in reducing PTSD symptoms. However, 2 studies of risperidone adjunctive therapy for treatment-resistant PTSD failed to demonstrate its superiority. One additional study showed that risperidone was better than placebo in reducing comorbid psychotic symptoms but not better in reducing PTSD symptoms. Despite some negative findings, several double-blind, randomized controlled trials (RCTs) have shown favorable results for risperidone as an effective treatment for PTSD.46 Intrusive and hypervigilance symptom subscales showed the greatest improvement when atypical antipsychotics were used for PTSD.47 Although the mechanism of action of atypical antipsychotics in the treatment of PTSD remains incompletely understood, they are believed to improve PTSD symptoms and exert an anxiolytic effect by affecting the dopaminergic and serotonergic systems and by blocking the α-1 adrenoreceptor.48 In addition, these medications may reduce psychotic symptoms associated with PTSD by blocking dopamine receptors.47 Atypical antipsychotics are also antihistaminic, which can improve sleep and nightmares that frequently occur in PTSD.49
Use of selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for the treatment of PTSD in those with bipolar disorder is limited by their potential to induce a manic/hypomanic episode or to promote rapid mood cycling3; rates of antidepressant-induced mood cycling range from 20% to greater than 50%.50,51 Therefore, the selection of an antidepressant for the treatment of PTSD in those with bipolar disorder warrants caution, given the potential destabilizing influence of antidepressants on mood. Adrenergic inhibitors, such as β-adrenergic blockers (eg, propranolol), α-2 adrenergic agonists (eg, clonidine), and α-1 antagonists (eg, prazosin) have been reported to reduce PTSD-related symptoms (including anxiety, irritability, sleep disturbance, and nightmares) associated with PTSD.3 Although the effects of these medications on bipolar disorder have not been systematically assessed, these medications are unlikely to exacerbate mood cycling.52 Benzodiazepines are commonly used as adjunctive therapy for the treatment of bipolar disorder and anxiety disorders. However, the overall efficacy of benzodiazepines for the treatment of PTSD tends to be low.53 Evidence suggests that benzodiazepines used during the acute post-trauma period may be associated with an increased likelihood of developing PTSD over time.54,55 Due to the lack of systematic studies addressing the efficacy of medications for those with comorbid bipolar disorder and PTSD, it is reasonable to optimize mood stabilizers and consider augmentation with adrenergic inhibitors or atypical antipsychotics before using antidepressants in this population.3
Treatment nonadherence can pose an issue for those with comorbid bipolar disorder and PTSD. Due to shared risk factors between bipolar disorder and PTSD, the characteristics that predict nonadherence in one population are often present in the other, suggesting a high likelihood of treatment nonadherence in those with coexisting bipolar disorder and PTSD.56 Nonadherence may be related to the trauma-related interpretations attributed to interactions with their physicians and their prescribed medications in those with bipolar disorder and PTSD who have suffered from early childhood trauma. Since treatments for bipolar disorder are usually associated with a high side effect burden and the need for lifelong adherence, clinicians should monitor individuals with comorbid bipolar disorder and PTSD closely for treatment nonadherence while being aware of patient-physician dynamics that might contribute to this behavior.56 It is recommended that clinicians should discuss reproductive health with patients diagnosed with comorbid bipolar disorder and PTSD, including the planning of pregnancy in the setting of medication use and the use of effective contraceptive methods.
Which Psychological Treatments Are Efficacious for Each Disorder When Bipolar Disorder and PTSD Coexist?
Evidence-based psychosocial treatments exist both for PTSD and bipolar disorder; however, treatment guidelines for this comorbidity are lacking. Several psychological interventions for PTSD (including prolonged exposure therapy, cognitive process therapy, psychodynamic therapy, and eye movement desensitization and reprocessing [EMDR] therapy) are efficacious and superior to control conditions.3,57 Current treatment guidelines for bipolar disorder indicate that combining psychological and psychopharmacologic treatments is optimal for bipolar disorder, while adjunctive psychological treatments are particularly effective for depressive symptoms.58
Psychological interventions that have the strongest evidence of efficacy include psychoeducation, CBT, family-focused psychotherapy, and interpersonal and social rhythm therapy.58,59 A recent meta-analysis of 39 RCTs of adjunctive therapies60 found that patients with bipolar disorder who were treated with both manualized psychotherapy and medications had fewer recurrences of mood episodes compared to those treated with psychopharmacology alone, with greater benefits noted for interventions that employed active skills training.
Despite this robust research on psychosocial interventions for PTSD and bipolar disorder, limited research exists on psychotherapies that target PTSD when PTSD and bipolar disorder coexist. Much of the existing literature calls for more research on this subject or lists bipolar disorder as an exclusion criterion. However, some case studies61,62 and larger trials suggest that positive results are found when targeting trauma symptoms in those with PTSD and bipolar disorder.
In an uncontrolled study,63 32 individuals with comorbid bipolar disorder and PTSD received 10 sessions of prolonged exposure. PTSD symptoms, including thoughts of suicide, were decreased at the end of treatment and at 6-month follow-up. Another study investigated the effects of EMDR in patients with bipolar I or II disorder with a history of traumatic events.64 Patients treated with EMDR showed improvements in trauma symptoms and mood stability; gains were largely maintained at 24-week follow-up.
Other studies lend further support for the positive effect on trauma patients in those with comorbid conditions. Mueser and colleagues1 investigated CBT for PTSD in patients with serious mental illness and found improvement in their trauma symptoms. Approximately one-fourth of the patients had comorbid PTSD and bipolar disorder, although the effects of PTSD treatment in this subgroup were not investigated. Deckersbach and colleagues65 investigated the effects of psychotherapy (eg, CBT, family-focused therapy, interpersonal social rhythm therapy) and collaborative care in 269 patients with bipolar disorder and anxiety spectrum disorders; of these, 45 had a history of comorbid PTSD and 14 had current PTSD. For patients with a history of PTSD and bipolar disorder, nearly two-thirds (63%) recovered with psychotherapy, and nearly one-half (44%) recovered with collaborative care (with a small-to-medium effect size). The results were similar for those with current PTSD. Results were not broken down by the specific psychotherapy used.
In addition to disorder-specific interventions, there is emerging evidence that dialectical behavior therapy (DBT) may be feasible, acceptable, and effective for treating symptoms of bipolar disorder66 and PTSD,67 particularly for those with a history of complex trauma and/or co-occurring personality pathology. DBT-based interventions may be beneficial in addressing certain difficulties that impact some patients with comorbid PTSD and bipolar disorder, including chronic emotional dysregulation, poor distress tolerance, and impulsive/self-destructive behaviors. More research is needed to assess this treatment in those with this specific comorbidity. In addition, there is emerging evidence that peer-based interventions, including individual and group support, may be helpful for patients with bipolar disorder and other psychiatric difficulties58,68; thus, these interventions may be useful in supplementing ongoing care. Overall, research suggests that psychotherapies that target trauma symptoms are efficacious in patients with comorbid PTSD and bipolar disorder. Existing research also suggests that these treatments are safe and accepted by patients, without evidence of mood symptom exacerbations or contraindications to trauma-focused treatment. However, more research involving different psychotherapies (eg, cognitive processing therapy and psychodynamic therapy) and with more rigorous methodologies (eg, larger sample sizes and control groups) is needed.
What Happened to Ms C?
After her initial evaluation, Ms C underwent medication changes, including initiation of a mood stabilizer, stopping the stimulant, and adjusting her antidepressant medication. After a discussion of mood stabilizing treatment options, lamotrigine was started at a dose of 25 mg daily and titrated up to 50 mg daily. She was advised to stop taking amphetamine dextroamphetamine due to its inducement of worsening mood instability. Her dose of citalopram was continued (at 20 mg daily) with a plan to taper and discontinue if mood instability persisted. She continued to work with her therapist to manage her trauma symptoms and panic disorder. She was advised to abstain from alcohol, given her history of heavy alcohol use. During follow-up, she reported a more stable mood and lessened anxiety and panic attacks while using lamotrigine (25 mg daily, as higher doses caused insomnia) and stopping her stimulant medication. The dose of lamotrigine was gradually increased (in 12.5-mg increments) to achieve a dose of 50 mg (with good effects on mood stability). She also limited her alcohol use and exercised regularly. Six months later, she complained of impulsively buying things she did not need (3 to 4 times a week), which led to an $18,000 bill and credit card debt. Subsequently, her citalopram was tapered and discontinued with the resolution of impulsivity and optimal mood stabilization while using lamotrigine (50 mg daily). Her PTSD symptoms remained in remission, and her anxiety/panic attacks were under good control without using as-needed lorazepam.
CONCLUSION
Studies examining PTSD in those with bipolar disorder report estimates as high as 40% for inpatient and community samples, with a lifetime prevalence of 16%, which is double that of PTSD in the general population; however, the etiology of comorbid bipolar disorder and PTSD remains incompletely understood. Symptoms of bipolar disorder and PTSD overlap; however, exposure to traumatic events is a key factor in the development of PTSD. The traumatic event may then lead to reexperiencing symptoms (eg, intrusive memories, nightmares, flashbacks, and hyperarousal) that were associated with the traumatic events. In contrast, bipolar disorder is characterized by mood episodes (including depression, hypomania, or mania) that are not necessarily triggered by traumatic events.
The pharmacologic treatment of comorbid bipolar disorder and PTSD poses unique challenges mainly due to side effects of the commonly used medications for one disorder that can worsen the symptoms of another disorder. For example, mood stabilizer treatments for bipolar disorder can worsen the cognitive symptoms in PTSD; similarly, antidepressants, the first-line treatment for PTSD, can induce mood switching and worsen mood stability in bipolar disorder. Other factors, such as treatment noncompliance, higher substance use, and increased risk of suicidality, need to be considered when treating comorbid bipolar disorder and PTSD. Initial data suggest that the use of a mood stabilizer, such as lamotrigine, could be effective in the treatment of PTSD, as it has been associated with a significant reduction in reexperiencing, avoidance, and numbing symptoms. Several double-blind RCTs have shown favorable results for risperidone as an effective treatment for PTSD with improvement in intrusive and hypervigilance symptom subscales. More systematic research is needed to establish the safety and efficacy of pharmacologic interventions in patients with bipolar disorder and PTSD.
Evidence-based psychosocial treatments exist both for bipolar disorder and PTSD; however, treatment guidelines for this comorbidity are lacking. Psychological treatments (including CBT, family-focused psychotherapy, and interpersonal and social rhythm therapy) often alleviate mood symptoms in bipolar disorder, whereas prolonged exposure therapy, cognitive process therapy, psychodynamic therapy, and EMDR therapy are effective psychotherapy interventions for PTSD. Initial data suggest that psychological interventions, including prolonged exposure therapy, EMDR therapy, and DBT, show promise in alleviating PTSD and mood symptoms. Overall, research suggests that psychotherapies that target trauma symptoms are safe and efficacious in patients with comorbid PTSD and bipolar disorder without evidence of mood symptom exacerbations or contraindications to trauma-focused treatment. However, more research involving different psychotherapies (eg, cognitive processing therapy and psychodynamic therapy) and with more rigorous methodologies (eg, larger sample sizes and control groups) is needed.
Article Information
Published Online: December 24, 2024. https://doi.org/10.4088/PCC.24f03768
© 2024 Physicians Postgraduate Press, Inc.
Submitted: May 15, 2024; accepted September 29, 2024.
To Cite: Chopra A, Matta SE, Vyas CM, et al. Comorbid bipolar disorder and posttraumatic stress disorder: clinical implications and management. Prim Care Companion CNS Disord. 2024;26(6):24f03768.
Author Affiliations: Department of Psychiatry, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts (all authors).
Corresponding Author: Amit Chopra, MBBS, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114 ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
Clinical Points
- Since bipolar disorder and posttraumatic stress disorder (PTSD) are highly comorbid conditions, distinguishing between them requires detailed knowledge of the clinical symptoms and history.
- Pharmacologic management of comorbid bipolar disorder and PTSD poses unique challenges, as side effects of the commonly used medications for one disorder can worsen the symptoms of another.
- Evidence-based psychosocial treatments exist both for bipolar disorder and PTSD; however, treatment guidelines for this comorbidity are lacking.
- A multidisciplinary and collaborative care approach that involves mental health professionals with expertise in treating both bipolar disorder and PTSD is key for optimizing outcomes and enhancing the overall quality of life for individuals with these psychiatric comorbidities.
References (68)

- Mueser KT, Rosenberg SD, Xie H, et al. A randomized controlled trial of cognitive behavioral treatment for posttraumatic stress disorder in severe mental illness. J Consult Clin Psychol. 2008;76(2):259–271. PubMed CrossRef
- Kessler RC, Rubinow DR, Holmes C, et al. The epidemiology of DSM-III-R bipolar I disorder in a general population survey. Psychol Med. 1997;27:1079–1089. PubMed CrossRef
- Otto MW, Perlman CA, Wernicke R, et al. Posttraumatic stress disorder in patients with bipolar disorder: a review of prevalence, correlates, and treatment strategies. Bipolar Disord. 2004;6(6):470–479. PubMed CrossRef
- Garno JL, Goldberg JF, Ramirez PM, et al. Impact of childhood abuse on the clinical course of bipolar disorder. Br J Psychiatry. 2005;186:121–125. PubMed CrossRef
- Neria Y, Olfson M, Gameroff MJ, et al. Trauma exposure and posttraumatic stress disorder among primary care patients with bipolar spectrum disorder. Bipolar Disord. 2008 Jun;10(4):503–510. PubMed CrossRef
- Assion HJ, Brune N, Schmidt N, et al. Trauma exposure and post-traumatic stress disorder in bipolar disorder. Soc Psychiatry Psychiatr Epidemiol. 2009;44(12):1041–1049. PubMed CrossRef
- VA/DoD Clinical practice guideline for management of posttraumatic stress disorder and acute stress disorder, version 4, 2023. Accessed November 21, 2024. https://www.healthquality.va.gov/guidelines/MH/ptsd/VA-DoD-CPGPTSD-Full-CPGAug242023.pdf
- Weathers FW, Litz BT, Keane TM, et al. The PTSD Checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD at www.ptsd.va.gov, 2024. Accessed November 21, 2024.
- American Psychiatric Association. Bipolar and Related Disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. 2022. Accessed November 21, 2024. https://doi.org/10.1176/appi.books.9780890425787.x03_Bipolar_and_Related_Disorders
- Bryant RA, Friedman MJ, Spiegel D, et al. A review of acute stress disorder in DSM-5. Depress Anxiety. 2011;28(9):802–817. PubMed CrossRef
- Goldstein RB, Smith SM, Chou SP, et al. The epidemiology of DSM-5 posttraumatic stress disorder in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions–III. Soc Psychiatry Psychiatr Epidemiol. 2016;51(8):1137–1148. PubMed CrossRef
- Young RC, Biggs JT, Ziegler VE, et al. Young Mania Rating Scale. Handbook of Psychiatric Measures. 2000:540–542.
- Kroenke K, Spitzer RL. The PHQ-9: a new depression and diagnostic severity measure. Psychiatr Ann. 2002;32:509–521.
- Cerimele JM, Bauer AM, Fortney JC, et al. Patients with co-occurring bipolar disorder and posttraumatic stress disorder: a rapid review of the literature. J Clin Psychiatry. 2017;78(5):e506–e514. CrossRef
- Hernandez JM, Cordova MJ, Ruzek J, et al. Presentation and prevalence of PTSD in a bipolar disorder population: a STEP-BD examination. J Affect Disord. 2013;150(2):450–455. PubMed CrossRef
- Aas M, Henry C, Andreassen OA, et al. The role of childhood trauma in bipolar disorders. Int J Bipolar Disord. 2016;4(1):2. PubMed CrossRef
- Etain B, Henry C, Bellivier F, et al. Beyond genetics: childhood affective trauma in bipolar disorder. Bipolar Disord. 2008;10(8):867–876. PubMed CrossRef
- Passos IC, Jansen K, Cardoso TdA, et al. Clinical outcomes associated with comorbid posttraumatic stress disorder among patients with bipolar disorder. J Clin Psychiatry. 2016;77(5):e555–e560. PubMed CrossRef
- Quarantini LC, Miranda-Scippa A, Nery-Fernandes F, et al. The impact of comorbid posttraumatic stress disorder on bipolar disorder patients. J Affect Disord. 2010;123(1–3):71–76. PubMed CrossRef
- Carter JM, Arentsen TJ, Cordova MJ, et al. Increased suicidal ideation in patients with co-occurring bipolar disorder and post-traumatic stress disorder. Arch Suicide Res. 2017;21(4):621–632. CrossRef
- Katz D, Petersen T, Amado S, et al. An evaluation of suicidal risk in bipolar patients with comorbid posttraumatic stress disorder. J Affect Disord. 2020;266:49–56. PubMed CrossRef
- Chengappa KN, Levine J, Gershon S, et al. Lifetime prevalence of substance or alcohol abuse and dependence among subjects with bipolar I and II disorders in a voluntary registry. Bipolar Disord. 2000;2(3 Pt 1):191–195. PubMed CrossRef
- Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511–2518. PubMed
- Kolodziej ME, Griffin ML, Najavits LM, et al. Anxiety disorders among patients with co-occurring bipolar and substance use disorders. Drug Alcohol Depend. 2005;80(2):251–257. PubMed CrossRef
- Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry. 2004;161(12):2222–2229. PubMed CrossRef
- Otto MW, Simon NM, Wisniewski SR, et al. Prospective 12-month course of bipolar disorder in out-patients with and without comorbid anxiety disorders. Br J Psychiatry. 2006;189:20–25. CrossRef
- Thatcher JW, Marchand WR, Thatcher GW, et al. Clinical characteristics and health service use of veterans with comorbid bipolar disorder and PTSD. Psychiatr Serv. 2007;58(5):703–707. PubMed CrossRef
- Russell SE, Wrobel AL, Skvarc D, et al. The impact of posttraumatic stress disorder on pharmacologic intervention outcomes for adults with bipolar disorder: a systematic review. Int J Neuropsychopharmacol. 2023;26(1):61–69. CrossRef
- Pacchiarotti I, Bond DJ, Baldessarini RJ, et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am J Psychiatry. 2013;170(11):1249–1262. PubMed CrossRef
- Lopes R, Fernandes L. Bipolar disorder: clinical perspectives and implications with cognitive dysfunction and dementia. Depress Res Treat. 2012;2012:275957. PubMed CrossRef
- Dubovsky SL, Marshall D. Benzodiazepines remain important therapeutic options in psychiatric practice. Psychother Psychosom. 2022;91(5):307–334. CrossRef
- Paton C. Benzodiazepines and disinhibition: a review. Psychiatr Bull. 2002;26(12):460–462. CrossRef
- Bryant RA. Post-traumatic stress disorder: a state-of-the-art review of evidence and challenges. World Psychiatry. 2019;18(3):259–269. PubMed CrossRef
- Simjanoski M, Patel S, Boni R, et al. Lifestyle interventions for bipolar disorders: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2023;152:105257. CrossRef
- Bojic S, Becerra R. Mindfulness-based treatment for bipolar disorder: a systematic review of the literature. Eur J Psychol. 2017;13(3):573–598. PubMed CrossRef
- Trauma-Informed Care in Behavioral Health Services. Treatment Improvement Protocol (TIP) Series, No. 57. Center for Substance Abuse Treatment. Substance Abuse and Mental Health Services Administration; 2014.
- Webber M, Fendt-Newlin M. A review of social participation interventions for people with mental health problems. Soc Psychiatry Psychiatr Epidemiol. 2017;52(4):369–380. CrossRef
- Cakir S, Tasdelen Durak R, Ozyildirim I, et al. Childhood trauma and treatment outcome in bipolar disorder. J Trauma Dissociation. 2016;17:397–409. PubMed CrossRef
- Caldieraro MA, Dufour S, Sylvia LG, et al. Treatment outcomes of acute bipolar depressive episode with psychosis. Depress Anxiety. 2018;35:402–410. PubMed CrossRef
- Hertzberg MA, Butterfield MI, Feldman ME, et al. A preliminary study of lamotrigine for the treatment of posttraumatic stress disorder. Biol Psychiatry. 1999;45(9):1226–1229. PubMed CrossRef
- Fesler FA. Valproate in combat-related posttraumatic stress disorder. J Clin Psychiatry. 1991;52(9):361–364. PubMed
- Lipper S, Davidson JR, Grady TA, et al. Preliminary study of carbamazepine in post-traumatic stress disorder. Psychosomatics. 1986;27(12):849–854. PubMed CrossRef
- Keck PE, McElroy SL, Friedman LM. Valproate and carbamazepine in the treatment of panic and posttraumatic stress disorders, withdrawal states, and behavioral dyscontrol syndromes. J Clin Psychopharmacol. 1992;12(1):36s–41s. CrossRef
- Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry. 2002;26:1035–1039. PubMed CrossRef
- Malek-Ahmadi P, Hanretta AT. Possible reduction in posttraumatic stress disorder symptoms with oxcarbazepine in a patient with bipolar disorder. Ann Pharmacother. 2004;38(11):1852–1854. PubMed CrossRef
- Wang HR, Woo YS, Bahk WM. Atypical antipsychotics in the treatment of posttraumatic stress disorder. Clin Neuropharmacol. 2013;36(6):216–222. PubMed CrossRef
- Ahearn EP, Juergens T, Cordes T, et al. A review of atypical antipsychotic medications for posttraumatic stress disorder. Int Clin Psychopharmacol. 2011;26(4):193–200. PubMed CrossRef
- Krystal JH, Neumeister A. Noradrenergic and serotonergic mechanisms in the neurobiology of posttraumatic stress disorder and resilience. Brain Res. 2009;1293:13–23. PubMed CrossRef
- Berger W, Mendlowicz MV, Marques-Portella C, et al. Pharmacologic alternatives to antidepressants in posttraumatic stress disorder: a systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(2):169–180. PubMed CrossRef
- Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179–184. PubMed CrossRef
- Bauer MS, Kurtz JW, Rubin LB, et al. Mood and behavioral effects of four-week light treatment in winter depressives and controls. J Psychiatr Res. 1994;28(2):135–145. PubMed CrossRef
- Giannini AJ, Pascarzi GA, Loiselle RH, et al. Comparison of clonidine and lithium in the treatment of mania. Am J Psychiatry. 1986;143(12):1608–1609. PubMed CrossRef
- Penava SJ, Otto MW, Pollack MH, et al. Current status of pharmacotherapy for PTSD: an effect size analysis of controlled studies. Depress Anxiety. 1996;4(5):240–242.
- Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry. 1996;57(9):390–394. PubMed
- Mellman TA, Bustamante V, David D, et al. Hypnotic medication in the aftermath of trauma. J Clin Psychiatry. 2002;63(12):1183–1184. PubMed CrossRef
- Rakofsky JJ, Levy ST, Dunlop BW. Conceptualizing treatment nonadherence in patients with bipolar disorder and PTSD. CNS Spectr. 2011;16(1):11–20. PubMed CrossRef
- Watts BV, Schnurr PP, Mayo L, et al. Meta-analysis of the efficacy of treatments for posttraumatic stress disorder. J Clin Psychiatry. 2013;74(6):11710.
- Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97–170. PubMed CrossRef
- Nierenberg AA, Agustini B, Köhler-Forsberg O, et al. Diagnosis and treatment of bipolar disorder: a review. JAMA. 2023;330(14):1370–1380. PubMed
- Miklowitz DJ, Efthimiou O, Furukawa TA, et al. Adjunctive psychotherapy for bipolar disorder: a systematic review and component network meta-analysis. JAMA Psychiatry. 2021;78(2):141–150. CrossRef
- Moring JC, Koch LM, Cherrington A, et al. Cognitive processing therapy for PTSD and bipolar disorder comorbidity: a case study. Cogn Behav Pract. 2022;29(2):425–433. CrossRef
- Hori A, Takebayashi Y, Tsubokura M, et al. Case report: PTSD and bipolar II disorder in Fukushima disaster relief workers after the 2011 nuclear accident. BMJ Case Rep. 2020;13(9):e236725. CrossRef
- Katz D, Petersen T, Rabideau DJ, et al. A trial of prolonged exposure therapy for outpatients with comorbid bipolar disorder and posttraumatic stress disorder (PTSD). J Affect Disord. 2024;344:432–439. CrossRef
- Novo P, Landin-Romero R, Radua J, et al. Eye movement desensitization and reprocessing therapy in subsyndromal bipolar patients with a history of traumatic events: a randomized, controlled pilot-study. Psychiatry Res. 2014;219(1):122–128. PubMed CrossRef
- Deckersbach T, Peters AT, Sylvia L, et al. Do comorbid anxiety disorders moderate the effects of psychotherapy for bipolar disorder? Results from STEP-BD. Am J Psychiatry. 2014;171(2):178–186. PubMed CrossRef
- Jones BDM, Umer M, Kittur ME, et al. A systematic review on the effectiveness of dialectical behavior therapy for improving mood symptoms in bipolar disorders. Int J Bipolar Disord. 2023;11(1):6. CrossRef
- Harned MS, Korslund KE, Foa EB, et al. Treating PTSD in suicidal and self-injuring women with borderline personality disorder: development and preliminary evaluation of a Dialectical Behavior Therapy Prolonged Exposure Protocol. Behav Res Ther. 2012;50(6):381–386. PubMed CrossRef
- Lloyd Evans B, Mayo Wilson E, Harrison B, et al. A systematic review and meta analysis of randomised controlled trials of peer support for people with severe mental illness. BMC Psychiatry. 2014;14:39. PubMed
This PDF is free for all visitors!



