Trichotillomania (TTM) is a disorder characterized by recurrent episodes of hair pulling that affects a growing and diverse patient population. The behavior is a result of conscious or unconscious stimuli aimed at alleviating stress. TTM can be diagnosed, typically by a psychiatrist or dermatologist, with various assessment tools and scales. Although researchers continue to discover new pharmacologic regimens and nonpharmacologic therapies, there is no single, effective, US Food and Drug Administration-approved option available for patients. Treatment of TTM with the least occurrence of relapse consists of a combination of pharmacologic and nonpharmacologic options and calls for the involvement of a multidisciplinary team along with family members and friends. This review provides an analysis of the current treatment modalities in the management of TTM and highlights the need for further epidemiologic, genetic, neuroimaging, and dietary research to better understand the complicated nature of the disorder.’ ‹
Therapeutic Aspects of Trichotillomania:
A Review of Current Treatment Options
ABSTRACT
Trichotillomania (TTM) is a disorder characterized by recurrent episodes of hair pulling that affects a growing and diverse patient population. The behavior is a result of conscious or unconscious stimuli aimed at alleviating stress. TTM can be diagnosed, typically by a psychiatrist or dermatologist, with various assessment tools and scales. Although researchers continue to discover new pharmacologic regimens and nonpharmacologic therapies, there is no single, effective, US Food and Drug Administration–approved option available for patients. Treatment of TTM with the least occurrence of relapse consists of a combination of pharmacologic and nonpharmacologic options and calls for the involvement of a multidisciplinary team along with family members and friends. This review provides an analysis of the current treatment modalities in the management of TTM and highlights the need for further epidemiologic, genetic, neuroimaging, and dietary research to better understand the complicated nature of the disorder.
Prim Care Companion CNS Disord 2018;20(6):18nr02344
To cite: Jafferany M, Patel A. Therapeutic aspects of trichotillomania:
a review of current treatment options. Prim Care Companion CNS Disord. 2018;20(6):18nr02344.
To share: https://doi.org/10.4088/PCC.18nr02344
© Copyright 2018 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry, Central Michigan University College of Medicine, Saginaw, Michigan
*Corresponding author: Mohammad Jafferany, MD, FAPA, Department of Psychiatry, Central Michigan University College of Medicine, 3215 Hallmark Ct, Saginaw, MI 48603 ([email protected]).
Trichotillomania (TTM) is a disorder characterized by hair pulling and is one of the primary diseases studied in the field of trichopsychodermatology, a subspecialty of psychodermatology. Trichopsychodermatology aims to gain a comprehensive view of the psychosocial impact of hair disorders, impact of stress on hair loss, and reduction of other comorbid psychological conditions to improve quality of life.1 Due to the impact on appearance, there is often decreased self-confidence associated with TTM, which has led to social stigma, underreporting, mistreatment, and incomplete treatment.2
EPIDEMIOLOGY AND PREVALENCE
There is a lack of substantial epidemiologic research on TTM to date. Studies have shown varying results with respect to epidemiologic characteristics such as prevalence of chronic or acute TTM. The mean age at onset for hair-pulling symptoms has been reported as bimodal, occurring in either early childhood or adolescence.3 The adolescent or later onset of TTM has been found to be more severe and resistant to treatment methods compared to childhood onset.4 Although the female-to-male ratio of disease is 4:1, in children the ratio is more equal.5 TTM can manifest at any site on the body where hair is located. The most common sites of hair pulling are the scalp (72.8%), eyelashes, and eyebrows (56.4%) followed by pubic hair (50.7%).6 Less-common sites include body and facial hair.
TTM can be chronic in many patients, and there is a common presence of comorbid conditions like nail biting, skin picking, headache, trichobezoar, carpal tunnel syndrome, and scalp injury.7 Patients seeking psychiatric care who are suspected to have TTM must meet 5 criteria as established by the DSM-5 during the diagnostic interview and history-gathering portion of the visit. Patients should be appropriately screened for other psychiatric illnesses due to the high occurrence of comorbid conditions with TTM, specifically depression (70% comorbidity) and substance abuse (17.7% comorbidity of tobacco product use and 14.1% comorbidity of alcohol use).6 Age can be an important potential indicator of comorbid conditions. Kessler et al8 found that adolescents and adults with TTM have a higher incidence of mental disorders, while preadolescents with TTM have shown little psychopathological involvement.
The 2 types of hair pulling are either conscious or unconscious in nature. The autonomic/habitual type comprises 5%–47% of patients and involves attention focused away from the actual area of hair pulling. The focused/compulsive type comprises 15%–34% of patients who direct attention on the act of hair pulling itself.9 The focused form of TTM involves the conscious, purposeful pulling of hair usually mediated with heightened anxiety and stress. There are several triggers for hair pulling, which could be classified into sensory (hair thickness, length, location, and physical sensation on the scalp), emotional (feelings of anxiousness, boredom, anger, and frustration), or cognitive (thoughts about the appearance of hair).10 Psychosocial dysfunction is common in patients with TTM. Many with the disorder have low self-esteem, depression, guilt, anxiety, and shame, with an overall lower reported quality of life compared to the general population.11
DIFFERENTIAL DIAGNOSIS AND COMORBIDITIES
Many disorders present with hair loss and may appear similar to TTM. It is important to distinguish acquired from congenital causes, presence of scarring, and the pattern of hair loss (diffuse, patchy, focal). Specific causes of hair loss that are similar to TTM in that they are acquired, nonscarring (unless chronic damage is present), and have a patchy pattern are alopecia areata, tinea capitis, and androgenic alopecia.12
Obsessive-compulsive disorder (OCD) is characterized by obsessions (stress and anxiety inducing persistent, intrusive, and unwanted thoughts, images, or doubts) and compulsions (ritualistic/repetitive behaviors that are done to lower the stress that is associated with obsessions). OCD is significantly more prevalent in patients with TTM than in the general population and ranges from 13%–27% in reported studies.10 In contrast, patients with OCD have a lower incidence of TTM at 5%–7%.11 Females are more likely to have TTM than males and are also more likely to have other body-focused repetitive behavior disorders like skin picking and nail biting. The presence of a first-degree relative with a body-focused repetitive behavior disorder is also more common in these female patients.11 In contrast, males are twice as likely to have obsessive-compulsive spectrum disorder. Specifically, there has been a greater incidence of body dysmorphic disorder, hypochondriasis, chronic motor tics, and Tourette’s disorder in males with TTM.11
Body dysmorphic disorder can be included in the differential diagnosis of TTM. Body dysmorphic disorder is characterized by obsessions and perceptions about a perceived defect of one’s physical appearance. Although hair pulling can manifest in patients with body dysmorphic disorder, the motivation behind the habit is to correct a perceived physical defect. Tourette’s disorder shares similarities with TTM such as underlying sensory cues and structural abnormalities found in magnetic resonance imaging scans.
PATHOPHYSIOLOGY
The pathophysiology underlying TTM has been debated, with no overarching consensus formed among researchers and physicians. Although TTM is currently classified under the OCD spectrum of disorders, there are many other proposed models including the behavioral model, which characterizes hair-pulling behavior under the tension reduction theory in which a coping behavior develops in response to stress and is reinforced by the reduction of stress. The psychoanalytic model explains TTM as a result of unconscious conflicts from real or perceived threats. The biologic model studies TTM from a neurobiology perspective, with a focus on neuroanatomical identification of specific areas of the brain that display abnormalities.
ASSESSMENT TOOLS, SCREENING,
SCALES, AND DIAGNOSIS
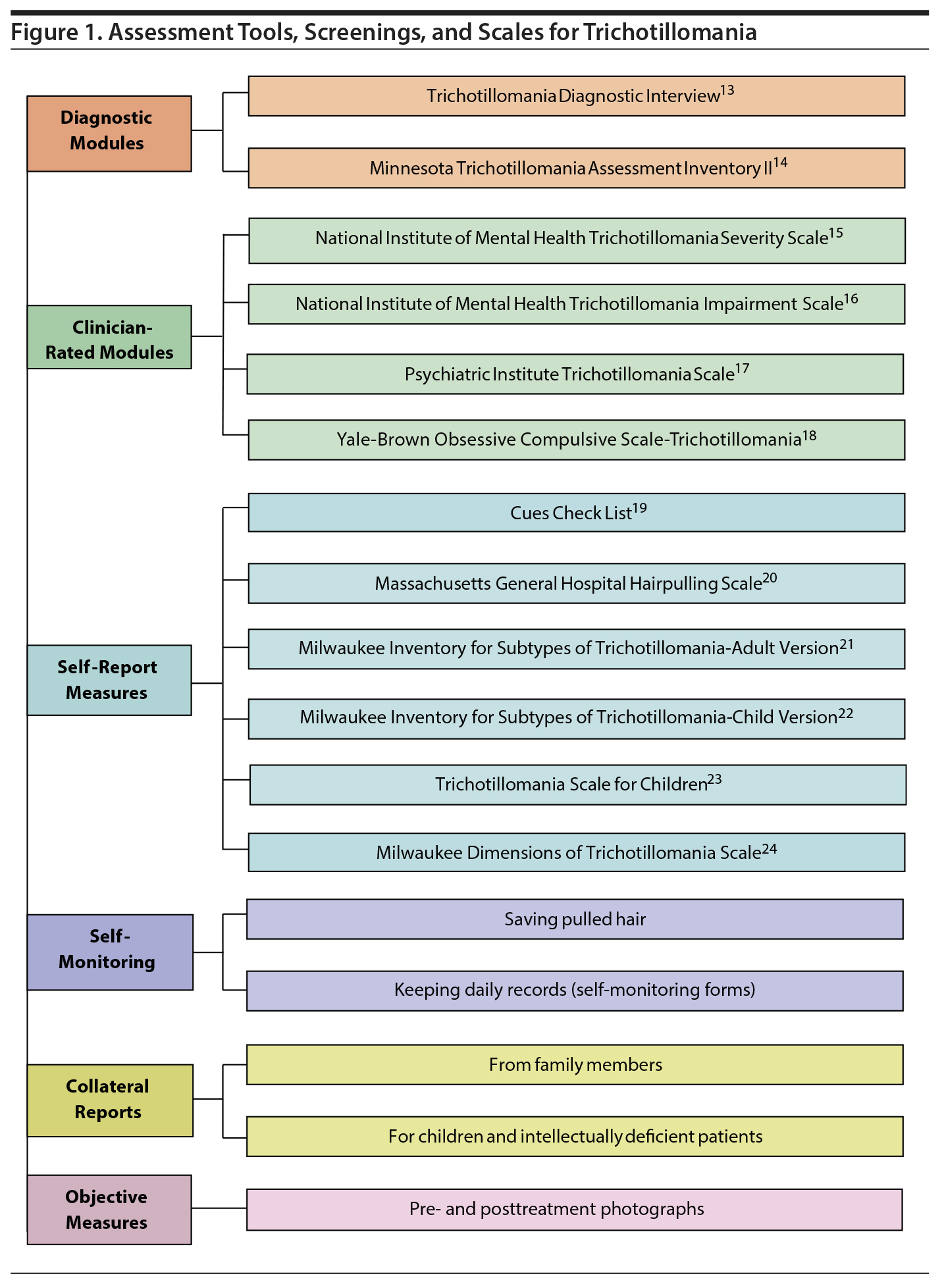
TTM is chronic in nature with fluctuations in intensity. Although TTM is not difficult to diagnose because of the specific patterns of behavior, many patients do not seek treatment due to embarrassment or feelings of shame and guilt. In a study6 examining 1,048 patients who met the diagnostic criteria for TTM, only 39.5% had received treatment from a therapist and only 27.3% had sought treatment from a psychiatrist. Specific assessments, screening, and scales implemented in the diagnosis of TTM are shown in Figure 1.13–24 In addition to the various screening forms available for TTM, there are also specific physical examination techniques and procedures that can be used to correctly diagnose TTM. These diagnostic techniques are shown in Figure 2 and are particularly helpful in distinguishing the disorder from other similarly appearing dermatologic conditions.
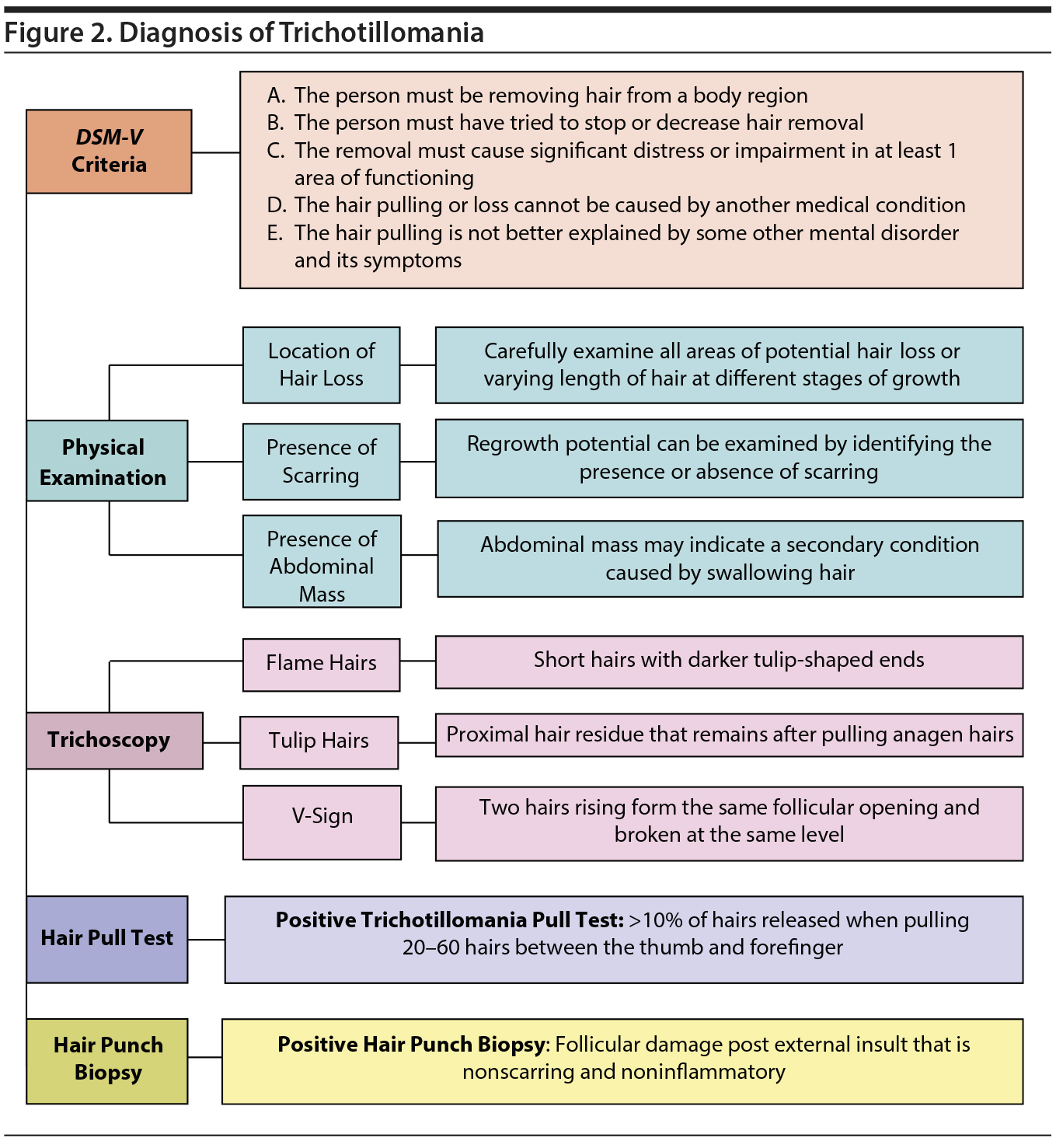
Some patients may not be fully transparent about their hair-pulling behavior; therefore, a thorough physical examination is vital. The physician should look at all areas of potential hair loss or varying length of hair at different stages of growth. Regrowth potential can be examined by identifying the presence or absence of scarring. The possibility of trichobezoar (abdominal mass from swallowing hair) should also be assessed with an abdominal examination.
Positive hair punch biopsy shows follicular damage post external insult that is nonscarring, noninflammatory alopecia.2 However, in patients with chronic TTM, without treatment the damage can transition from nonscarring to scarring, leading to permanent hair loss. Trichoscopy in TTM shows flame hairs (proximal hair residue that remains after pulling anagen hairs), V-sign (2 hairs rising from the same follicular opening and broken at the same level), and tulip hairs (short hairs with darker tulip-shaped ends). The Hair Pull Test12 is another assessment performed by pulling a bundle of 20–60 hairs between the thumb and forefinger from multiple locations. The result of the test is considered positive if > 10% of the hairs are released.
TREATMENT
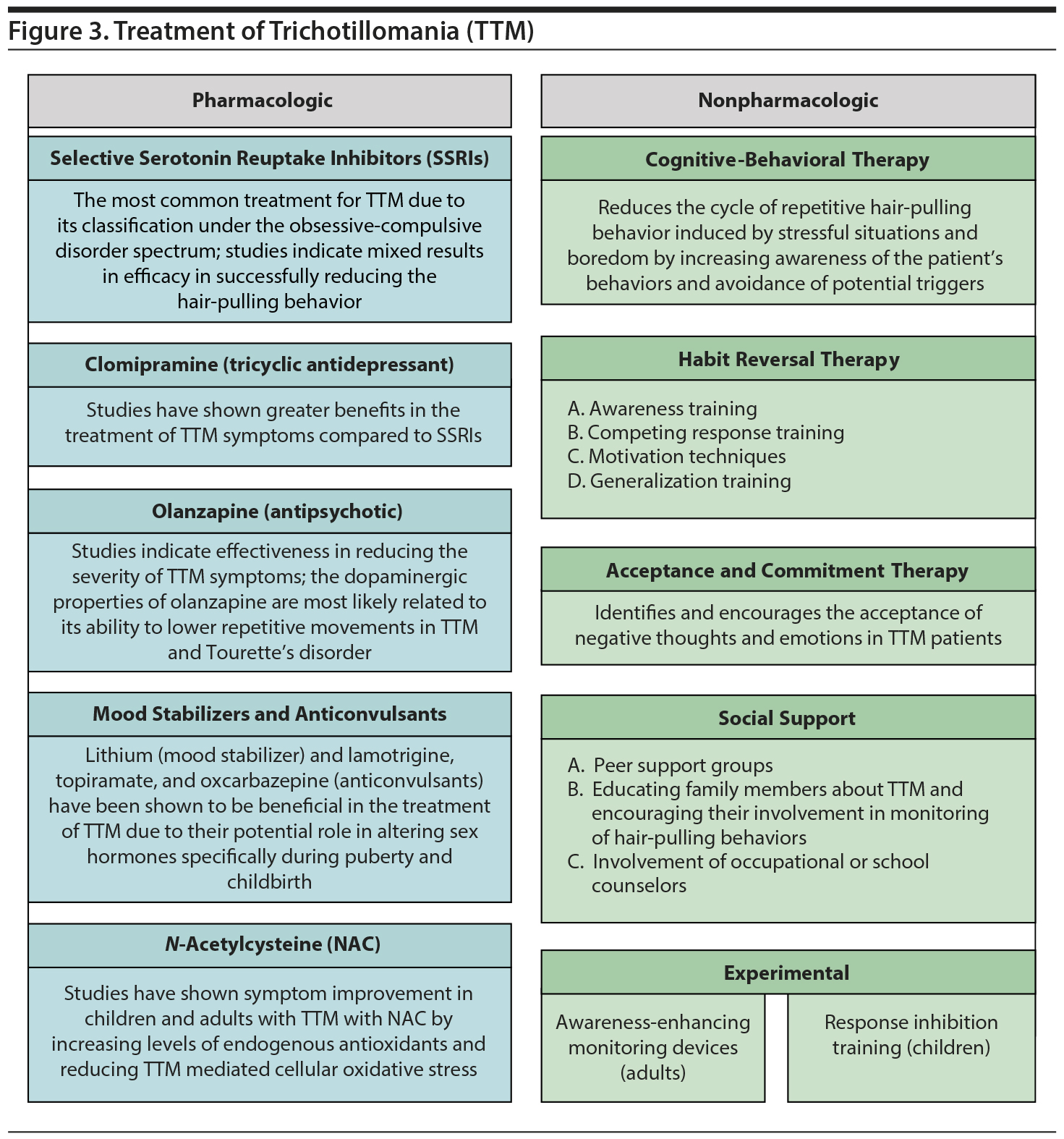
Treatment for TTM currently consists of a mixture of pharmacologic and nonpharmacologic (psychotherapeutic) methods as shown in Figure 3. Pharmacologic treatment includes lithium salts, tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), antipsychotics, and N-acetylcysteine (NAC). Psychotherapeutic treatments include habit reversal therapy (HRT), acceptance and commitment therapy, awareness-enhancing monitoring devices, and response inhibition training. Experimental therapies highlighted in this review have been administered to patients with varying success in multiple case studies.25 However, it is difficult to fully assess validity with the limited sample sizes and lack of additional studies with consistent data. In addition, it is important for physicians to monitor for the presence of potential adverse effects when administering medications like antipsychotics, anticonvulsants, and antidepressants. Treatment should follow a multidisciplinary approach and consist of follow-up to prevent relapse, assistance in the management of potential comorbid conditions, and the improvement of quality of life.7
Nonpharmacologic Treatment
A variety of psychotherapeutic techniques have been implemented in the treatment of TTM. The most commonly employed therapies are as follows.
TTM is characterized under the OCD spectrum of psychological disorders because of the obsessive, intrusive, persistent thoughts that induce stress and result in patients engaging in compulsive acts of hair pulling.26 Cognitive-behavioral therapy (CBT) has been shown to be very effective in the treatment of OCD-related disorders.26 Cognitive and neuropsychological components of TTM have been shown to be treatable with proper behavior therapy. Stressful situations and boredom lead many patients with TTM to develop the urge to pull hair: the increase in tension and stress that builds up manifests as hair-pulling behavior. After the patient engages in the practice of hair pulling, the tension diminishes, only to recur again in the future. This cycle can be modified through behavior therapy by proper identification and conscious awareness of potential stress-inducing triggers. To successfully implement CBT as a method of treatment, the protocol indicates the use of sessions aimed at planning and education related to symptoms, repeated exposures to the feared stimuli, and strategic attempts to eliminate the ritualistic behavior. Treatment typically involves 12–16 weekly sessions and “homework practice” sessions in between. In a study investigating the effectiveness of the cognitive and behavioral aspects of CBT, Keijsers et al27 found that both features were successful in reducing TTM symptoms in the categories of severity, urge, inability to resist, and negative beliefs by identifying and addressing the autonomic beliefs resulting in hair-pulling behavior. However, after a period of time without treatment, relapse occurred in many patients, which indicates the need for planned booster sessions.27
Group CBT has been shown to be beneficial in TTM because patients receive a larger amount of feedback and guidance through personal accounts that can lead to greater positive changes in symptoms compared with one-on-one CBT sessions. However, due to the lack of knowledge in the theoretical basis of group CBT and professional training in group techniques, it has not been implemented extensively as a treatment method.7
HRT shares essential principles of CBT but aims to reverse the positive reinforcement that patients with TTM have developed. By completing the therapy, patients learn to effectively monitor and increase awareness of their hair-pulling behavior. Cognitive restructuring methods are an essential component of HRT, which decrease the dysfunctional cognitions and off-balance emotional regulation that increase hair-pulling.28 The focus of HRT is to assist patients to reduce receptive unwanted behaviors by bringing them to conscious awareness and replacing them with alternative behaviors that are not bothersome and do not interfere with overall quality of life. The 4 components of HRT include awareness training, competing response training, motivational techniques and social support, and generalization training.28
Awareness training involves specific steps to increase self-control with regard to hair pulling by increasing patients’ awareness of their behavior. Specifically, patients can practice awareness training by techniques such as describing themselves carrying out an unwanted behavior while watching themselves in the mirror and being more mindful of specific stressful triggers of hair pulling. Family members, counselors, and therapists are also encouraged to point out when the patient engages in the behavior.29 Awareness training prepares patients for the next component of HRT, which involves developing a competing response, eliminating behaviors that occur immediately prior to hair pulling, and avoidance of stressful situations.
Competing response training assists in the development of behaviors that are different from those related to hair pulling specifically when the urges occur. The patient is taught to perform this replacement act whenever there are thoughts or engagement in hair pulling. An example of a replacement act can be to hold a fist with both hands to the side of the body whenever there is an urge or thought of hair pulling.29
Motivation techniques are important to implement after the successful formation of a replacement act for continued habit reversal and to prevent relapse. Habit inconvenience review is a method to motivate the patient to continue to avoid the unwanted behavior by brainstorming specific negative aspects attributed with it such as feelings of embarrassment, impact on work and social life, and general inconvenience.30 Social support procedure involves family members, school counselors, and close friends in the treatment process by praising the patient for the nonoccurence of the unwanted behavior. In addition, those offering social support are instructed to be attentive of instances when the patient may relapse and engage in the behavior and are encouraged to practice competing response with continued motivation.
Generalization training involves the symbolic reversal procedure wherein patients imagine themselves in stressful situations or triggers previously identified that typically result in them engaging in an unwanted behavior. They would be asked to imagine themselves starting the behavior but stopping without completion and committing to the competing behavior response instead.
Similar to CBT, relapse rates posttreatment are high with HRT. In addition, new information about the relationship between emotional regulation processes and the severity of TTM indicates that HRT does not target all the factors that contribute to the development, maintenance, and relapse of TTM.31 However, for many patients, HRT remains promising, and increased awareness of TTM and HRT as a treatment method should be stressed at a primary care and dermatologic level to more accurately determine its effectiveness.
Acceptance and commitment therapy (ACT) addresses the tendency of TTM patients to avoid unpleasant and aversive thoughts, sensations, and emotions (which lead them to pull hair). Researchers have found that patients who engage in avoidance of unwanted internal feelings through behaviors like hair pulling have more intense hair-pulling urges, lower control over the urges, and heightened overall distress from the behavior. These findings together indicate that TTM patients who exhibit avoidance have an overall lower quality of life. Through therapy, patients learn to be more mindful of their avoidance behaviors and increase the acceptance of these negative thoughts and emotions.
In a trial of 10 ACT sessions over 12 weeks, Rehm et al31 found that the therapy resulted in significant improvement of TTM severity and impairment in both self- and clinician-rated observations. Studies32 also indicate that, through ACT, there was significantly greater pre- to posttreatment reductions in comorbid conditions like depression and anxiety in patients with TTM.
The experimental awareness-enhancing monitoring device (combined with sessions of HRT) aims to increase awareness of hair-pulling behavior in patients with TTM and monitor and record these habits. A study by Himle et al33 recruited 21 adults with TTM who were assessed at baseline, at the end of the 9-session treatment, and 12 weeks posttreatment. The device, which is worn around the neck and both wrists, implements broadcasting signals and microprocessors to send vibrating alerts when the TTM patients draw their hands near their face and head. The vibration continues until the person turns it off by pressing a specific button. The results indicate a significant improvement of TTM symptoms and a positive reaction to the device by the participants.33
Response inhibition training is an experimental intervention developed from the connection found between TTM and response inhibition dysfunction. Specifically, the right-lateralized inferior frontal cortex is known as the central locus of inhibition, and networks like the cortical-striatal-thalamic-cortical circuit display structural abnormalities in patients with TTM.34 Lee et al35 conducted a pilot clinical trial of computerized cognitive training programs aimed at improving response inhibition and TTM symptoms in children (N = 22, 12 participated in the training and 10 were on the waitlist). Compared to control groups, response inhibition training showed a significantly higher response rate and lower level of hair pulling.35
Peer support groups and education of the family of TTM patients can also play an important role in improvement of symptoms. In addition, involvement of occupational and school counselors can assist patients and improve treatment success when combined with other options.36
Pharmacologic Treatment
No US Food and Drug Administration–approved treatments are currently available for TTM. However, a variety of medications have been used with varying success. Examples of commonly implemented pharmacologic treatments are as follows.
SSRIs are the most commonly used treatment for TTM. The underlying reasoning behind the use of SSRIs in patients with TTM is based on it being classified under the spectrum of OCD. However, TTM differs from OCD in that it is caused by strong urges that transform into feelings of satisfaction and gratification once the act of hair pulling is complete. Also, unlike OCD, there are no obsessions present before the compulsions, and TTM patients’ symptoms do not change over time in focus and severity.37
Although SSRIs are widely implemented in the treatment of TTM, varying results indicate the need for further research and better understanding of the disorder and mechanism of actions of treatment options. In a systematic review25 of the effectiveness of SSRIs, there was no significant difference found with respect to the benefit of SSRIs. However, further research is indicated regarding the particular types of SSRIs used in the treatment of TTM, as citalopram may be more effective than fluoxetine. In contrast, in a meta-analysis38 of the effects of serotonin reuptake inhibitors (SRIs) and behavioral therapy, researchers found that there was a moderate effect size with SRI use and a greater effect size with behavioral therapy (increases with greater number of contact hours), indicating such nonpharmacologic treatment may be more beneficial for patients compared to SRI administration. In an open-label trial studying the efficacy of the SSRI escitalopram, Gadde et al39 found that some patients had a significant improvement in TTM following the 12-week treatment period.
SSRIs are also the most frequently prescribed drugs for treatment of pediatric TTM, although their effectiveness in children is relatively unknown. In a review by Sah et al,40 the authors highlight the importance of completing more comprehensive studies of antidepressant medications with blinding, randomization, and placebo controls due to black box warnings and insufficient supporting evidence of efficacy. In addition, treatment options for patients with TTM should be determined based on the age at onset. For example, young children frequently “outgrow” habits like hair pulling over time and often require no intervention, while adolescents may benefit most from therapies that increase awareness of their behavior. Cognitive-behavioral therapy remains the treatment of choice in pediatric patients with TTM due to its safety and known efficacy.
The tricyclic antidepressant clomipramine has shown benefits in the treatment of TTM and improvements in symptoms compared to SSRIs despite their preferred and continued use.25 A study by Ninan et al41 compared clomipramine with CBT in the treatment of TTM and found statistically insignificant symptom reduction of clomipramine along with evidence of CBT outcompeting the medication in symptom improvement scores. Within the class of tricyclic antidepressants, there may be differences in the efficacy of medications, indicating the need for further research. For example, in a 10-week double-blind crossover trial of clomipramine and desipramine, Swedo et al42 found that clomipramine resulted in significantly greater improvement in symptoms compared to desipramine. Although moderately effective, clomipramine has an extensive side effect profile and varying patient adherence, and understanding of its long-term effectiveness is incomplete.43
Several antipsychotics have been studied and used in the treatment of TTM. For example, olanzapine, although known to have metabolic side effects such as weight gain, was shown to be effective in a study44 investigating its role in TTM treatment when compared to placebo. In the study,44 13 participants with TTM were given olanzapine and 12 were given placebo. The treatment group showed significant change from baseline to endpoint, with improvement in the severity of symptoms of TTM. The study44 further supports the theory that TTM has features unrelated to OCD and more specifically shares characteristics with repetitive movement disorders like Tourette’s disorder. The effectiveness of olanzapine may be related to its dopaminergic properties that also make it effective in the treatment of Tourette’s disorder.44 Quetiapine has also been reported to be successful in the treatment of TTM in case reports. In a report by Paholpak and Mendez,45 a patient who developed TTM 8 years into her diagnosis of dementia was successfully treated with quetiapine after SSRI administration was unsuccessful. In another case report by Junior et al,46 a patient with an 8-year history of TTM was successfully treated with quetiapine after being administered fluoxetine, which, although it decreased hair pulling, led to insomnia and weight loss. Similarly, aripiprazole has also been studied in the treatment of TTM. In an 8-week, open-label, flexible-dose trial47 consisting of 12 subjects, participants who were assessed 2 or more times were found to have a significant mean reduction in end points of TTM symptoms. In a case report by Sasaki and Iyo,48 low-dose aripiprazole was successful in treating puberty-onset TTM in a 14-year-old girl. Aripiprazole is considered a safer alternative to antidepressants when treating TTM in adolescents due to their increased risk of suicidal ideation. Other reports49,50 show the successful use of aripiprazole in the treatment of patients with TTM and comorbid conditions like restless leg syndrome and Huntington’s disease. These reports49,50 indicate the need for further studies investigating the properties of different classes of medications in the treatment of TTM in patients with specific comorbidities.
Mood stabilizers like lithium and anticonvulsants like lamotrigine, topiramate, and oxcarbazepine have been reported to be beneficial in the treatment of TTM. In cases of TTM with bipolar disorder following childbirth, Sharma et al51 found women had a decrease in hair-pulling symptoms after the administration of lithium or lamotrigine. To further support the role of sex hormones in TTM, they found that in 462 patients seeking TTM treatment, 94% were female, and the majority reported the onset of the hair-pulling behavior coincided with puberty. Some researchers point to the success of lithium and lamotrigine with regard to the role of sex hormones in the pathophysiology of TTM through the potential correlation of hair-pulling behavior during reproductive and hormonal changes in mice.52 Other anticonvulsants have also been found to be successful in TTM treatment such as in a case report in which oxcarbazepine was successful in treating a patient with TTM and comorbid binge-eating disorder.53 Also, in an open-label trial54 of the anticonvulsant topiramate, the medication was found to be successful in the reduction of TTM severity.
NAC is a cysteine-derived food additive that has been shown to be effective in the treatment of TTM with an unknown mechanism of action. NAC is used for the treatment of many medical conditions such as acetaminophen overdose, doxorubicin-induced cardiotoxicity, stable angina pectoris, ischemia reperfusion cardiac injury, acute respiratory distress syndrome, bronchitis, influenza, heavy metal toxicity, and chemotherapy-induced toxicity and as a mucolytic for chronic obstructive pulmonary disease.55 Due to the ability of NAC to impact so many pathways and its overall safe profile with side effects being mild at high doses (nausea, vomiting, diarrhea, and flatulence), it is used to treat various conditions across disciplines. The role that NAC plays in antioxidant, anti-inflammatory, and neurotransmitter modulatory pathways makes it important for study in many psychiatric conditions in which there is a dysregulation of these pathways such as bipolar depression, major depressive disorder, and schizophrenia.56,57
Proposed mechanisms indicate that since NAC is a precursor to the primary antioxidant made to protect the brain against reactive oxygen species (ROS), TTM may be caused by excessive oxidative stress. Specifically, accumulation of ROS from loss of antioxidants in the brain lead to neuronal damage that induces hair-pulling behavior.31 Also, OCD patients have been found to have abnormalities in glutamate (endogenous antioxidant) metabolism, which can be overcome with the use of NAC to reduce oxidative stress and cytotoxicity from excess glutamate levels.58
In a 12-week controlled trial comprised of 50 individuals with TTM, Grant et al59 found a significant improvement in hair-pulling symptoms after 9 weeks of treatment with NAC compared to placebo. Further, Barroso et al60 found NAC effective in improving TTM symptoms in an 11-year-old patient (1,200 mg/d for 3 months with modest improvement and complete regrowth with 1,800 mg/d). Additionally, Barroso et al60 indicate that although SSRIs are used for the treatment of TTM, the presence of side effects makes it important to find alternative treatment options like NAC. Another case report61 found that a 28-year-old man and 40-year-old woman with TTM both responded successfully to NAC treatment, and the 28-year-old man had recurrence of TTM symptoms when he was noncompliant with the medication. Rodrigues-Barata et al62 found NAC led to the successful elimination of symptoms and complete hair regrowth in 2 women aged 23 and 19 years, with complete hair regrowth in 2 and 3 months, respectively. Finally, a report by Ozcan and Seckin63 found NAC, used in the treatment of TTM in 2 females aged 14 and 30 years, to be well-tolerated and effective.
Although numerous pharmacologic treatment options have been successfully administered to patients with TTM, placebo response rates remain high. Grant et al64 raise the concern of high placebo response rates in pharmacologic interventions of TTM. The overall lack of ability to identify effective pharmacologic treatments for TTM may be a result of unknown predictors of placebo response, which are poorly understood when compared to responses in other psychiatric conditions. Specifically, to better predict placebo response in certain patients, Grant et al64 point to the importance of analyzing baseline demographics and clinical characteristics.
CONCLUSION
TTM presents primarily as excessive hair-pulling behavior that can be conscious or unconscious in nature. The disorder is studied under the field of trichopsychodermatology and is managed primarily by psychiatrists and dermatologists. With many advancements made to better understand the pathophysiologic basis of TTM, there is no ideal, accepted, or approved treatment for the disorder.
Treatments for TTM fall under both pharmacologic and nonpharmacologic categories. Although relapse has been shown to be a recognized issue in the implementation of nonpharmacologic therapies like CBT and HRT, their success with continued monitoring by professionals and family members has been shown. With respect to pharmacologic treatment, many medications have been extensively used in the successful elimination of hair-pulling symptoms in TTM. Currently, SSRIs are the most widely used medication despite substantial evidence of relapse and the availability of alternative medications with increased efficacy like tricyclic antidepressants, antipsychotics, mood stabilizers, anticonvulsants, and NAC. The majority of available data points to the treatment of TTM with the combination of pharmacologic and nonpharmacologic treatment with continued follow-up and monitoring as most beneficial in the management of hair-pulling symptoms.
It is imperative to improve protocols for existing drugs while continuing to explore novel treatment options due to the lack of universally accepted and approved treatment options for TTM. With the advancement of epidemiologic, genetic, neuroimaging, and dietary studies, it may be possible to gain the knowledge needed to better assist the patient population affected by TTM. In addition, further attention and exploration in making necessary changes in the classification and nomenclature of this disease are important. TTM should be regarded as hair-pulling disorder as suggested by the DSM-5 classification system or given a more descriptive term like neuromechanical alopecia.
To better assist the growing and diverse patient population presenting with TTM, it is essential to implement a multidisciplinary approach with dermatologists, psychiatrists, counselors, and even family members. With further awareness of medical professionals about the complicated nature of TTM and the various treatment options available, symptoms of TTM in patients can be diagnosed, treated, and managed in a more systematic and effective way.
Submitted: June 26, 2018; accepted August 24, 2018.
Published online: November 22, 2018.
Potential conflicts of interest: None.
Funding/support: None.
REFERENCES
1. França K. Trichotillomania in Trichopsychodermatology. In: França, K, Jafferany, M, eds. Trichotillomania (Hair Pulling Disorder): Clinical Characteristics, Psychological Interventions and Emotional Effects. Hauppauge, NY: Nova Publishing Company; 2018.
2. Pereyra AD, Saadabadi A. Trichotillomania. StatPearls. Treasure Island, FL: StatPearls Publishing; 2018.
3. Swedo SE, Rapoport JL. Annotation: trichotillomania. J Child Psychol Psychiatry. 1991;32(3):401–409. PubMed CrossRef
4. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am. 1992;15(4):777–790. PubMed CrossRef
5. Lewin AB, Piacentini J, Flessner CA, et al; TLC-SAB. Depression, anxiety, and functional impairment in children with trichotillomania. Depress Anxiety. 2009;26(6):521–527. PubMed
6. Woods DW, Flessner CA, Franklin ME, et al; Trichotillomania Learning Center-Scientific Advisory Board. The Trichotillomania Impact Project (TIP): exploring phenomenology, functional impairment, and treatment utilization. J Clin Psychiatry. 2006;67(12):1877–1888. PubMed CrossRef
7. Toledo EL, De Togni Muniz E, Brito AM, et al. Group treatment for trichotillomania: cognitive-behavioral therapy versus supportive therapy. J Clin Psychiatry. 2015;76(4):447–455. PubMed CrossRef
8. Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617–627. PubMed CrossRef
9. Jafferany M, Osuagwu FC. Trichotillomania: Basic Concepts. In: França K, Jafferany M, eds. Trichotillomania (Hair Pulling Disorder): Clinical Characteristics, Psychological Interventions and Emotional Effects. Hauppauge, NY: Nova Publishing Company; 2018.
10. Christenson GA. Trichotillomania: from prevalence to comorbidity. Psychiatr Times. 1995;12:44–48.
11. Odlaug BL, Kim SW, Grant JE. Quality of life and clinical severity in pathological skin picking and trichotillomania. J Anxiety Disord. 2010;24(8):823–829. PubMed CrossRef
12. Xu L, Liu KX, Senna MM. A practical approach to the diagnosis and management of hair loss in children and adolescents. Front Med (Lausanne). 2017;4(4):112. PubMed CrossRef
13. Diefenbach GJ, Tolin DF, Hannan S, et al. Trichotillomania: impact on psychosocial functioning and quality of life. Behav Res Ther. 2005;43(7):869–884. PubMed CrossRef
14. Enos S, Plante T. Trichotillomania: an overview and guide to understanding. J Psychosoc Nurs Ment Health Serv. 2001;39(5):10–18. PubMed
15. Diefenbach GJ, Tolin DF, Crocetto J, et al. Assessment of trichotillomania: a psychometric evaluation of hair-pulling scales. Psychopathol Behav Assess. 2005;27(3):169–178. CrossRef
16. Woods DW, Wetterneck CT, Flessner CA. A controlled evaluation of acceptance and commitment therapy plus habit reversal for trichotillomania. Behav Res Ther. 2006;44(5):639–656. PubMed CrossRef
17. Woods DW, Flessner C, Franklin ME, et al. Understanding and treating trichotillomania: what we know and what we don’t know. Psychiatr Clin North Am. 2006;29(2):487–501, ix. PubMed CrossRef
18. Woods DW, Houghton DC. Diagnosis, evaluation, and management of trichotillomania. Psychiatr Clin North Am. 2014;37(3):301–317. PubMed CrossRef
19. Keuthen NJ, Sprich SE. Utilizing DBT skills to augment traditional CBT for trichotillomania: an adult case study. Cognit Behav Pract. 2012;19(2):372–380. CrossRef
20. Keuthen NJ, Flessner CA, Woods DW, et al; Trichotillomania Learning Center Scientific Advisory Board. Factor analysis of the Massachusetts General Hospital Hairpulling Scale. J Psychosom Res. 2007;62(6):707–709. PubMed CrossRef
21. Flessner CA, Woods DW, Franklin ME, et al. The Milwaukee Inventory for Subtypes of Trichotillomania-Adult Version (MIST-A): development of an instrument for the assessment of “focused” and “automatic” hair pulling. J Psychopathol Behav Assess. 2008;30(1):20–30. CrossRef
22. Flessner CA, Woods DW, Franklin ME, et al. The Milwaukee Inventory for Styles of Trichotillomania-Child Version (MIST-C): initial development and psychometric properties. Behav Modif. 2007;31(6):896–918. PubMed CrossRef
23. Tolin DF, Diefenbach GJ, Flessner CA, et al; Trichotillomania Learning Center Scientific Advisory Board. The Trichotillomania Scale for Children: development and validation. Child Psychiatry Hum Dev. 2008;39(3):331–349. PubMed CrossRef
24. Himle JA, Perlman DM, Lokers LM. Prototype awareness enhancing and monitoring device for trichotillomania. Behav Res Ther. 2008;46(10):1187–1191. PubMed CrossRef
25. Bloch MH, Landeros-Weisenberger A, Dombrowski P, et al. Systematic review: pharmacological and behavioral treatment for trichotillomania. Biol Psychiatry. 2007;62(8):839–846. PubMed CrossRef
26. Abramowitz JS, Blakey SM, Reuman L, et al. New directions in the cognitive-behavioral treatment of OCD: theory, research, and practice. Behav Ther. 2018;49(3):311–322. PubMed CrossRef
27. Keijsers GP, Maas J, van Opdorp A, et al. Addressing self-control cognitions in the treatment of trichotillomania: a randomized controlled trial comparing cognitive therapy to behaviour therapy. Cognit Ther Res. 2016;40(4):522–531. PubMed CrossRef
28. Morris SH, Zickgraf HF, Dingfelder HE, et al. Habit reversal training in trichotillomania: guide for the clinician. Expert Rev Neurother. 2013;13(9):1069–1077. PubMed CrossRef
29. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26(2):123–131. PubMed CrossRef
30. Azrin NH, Nunn RG. Habit-reversal: a method of eliminating nervous habits and tics. Behav Res Ther. 1973;11(4):619–628. PubMed CrossRef
31. Rehm I, Moulding R, Nedeljkovic M. Psychological treatments for trichotillomania: update and future directions. Australas Psychiatry. 2015;23(4):365–368. PubMed CrossRef
32. Vieira GLT, Lossie AC, Lay DC Jr, et al. Preventing, treating, and predicting barbering: a fundamental role for biomarkers of oxidative stress in a mouse model of Trichotillomania. PLoS One. 2017;12(4):e0175222. PubMed CrossRef
33. Himle JA, Bybee D, O’Donnell LA, et al. Awareness enhancing and monitoring device plus habit reversal in the treatment of trichotillomania: an open feasibility trial. J Obsessive Compuls Relat Disord. 2018;16:14–20. PubMed CrossRef
34. Mataix-Cols D, van den Heuvel OA. Common and distinct neural correlates of obsessive-compulsive and related disorders. Psychiatr Clin North Am. 2006;29(2):391–410, viii. PubMed CrossRef
35. Lee HJ, Espil FM, Bauer CC, et al. Computerized response inhibition training for children with trichotillomania. Psychiatry Res. 2018;262:20–27. PubMed CrossRef
36. Raj KS, Williams N, DeBattista C. Psychiatric disorders. In: McPhee SJ, Papadakis MA, Rabow MW, eds. Current Medical Diagnosis & Treatment 2010. New York, NY: McGraw-Hill Medical; 2010:5.
37. Shoenfeld N, Rosenberg O, Kotler M, et al. Tricotillomania: pathopsychology theories and treatment possibilities. Isr Med Assoc J. 2012;14(2):125–129. PubMed
38. McGuire JF, Ung D, Selles RR, et al. Treating trichotillomania: a meta-analysis of treatment effects and moderators for behavior therapy and serotonin reuptake inhibitors. J Psychiatr Res. 2014;58:76–83. PubMed CrossRef
39. Gadde KM, Ryan Wagner H 2nd, Connor KM, et al. Escitalopram treatment of trichotillomania. Int Clin Psychopharmacol. 2007;22(1):39–42. PubMed
40. Sah DE, Koo J, Price VH. Trichotillomania. Dermatol Ther (Heidelb). 2008;21(1):13–21. PubMed CrossRef
41. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61(1):47–50. PubMed CrossRef
42. Swedo SE, Leonard HL, Rapoport JL, et al. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). N Engl J Med. 1989;321(8):497–501. PubMed CrossRef
43. Walsh KH, McDougle CJ. Trichotillomania: presentation, etiology, diagnosis and therapy. Am J Clin Dermatol. 2001;2(5):327–333. PubMed CrossRef
44. Van Ameringen M, Mancini C, Patterson B, et al. A randomized, double-blind, placebo-controlled trial of olanzapine in the treatment of trichotillomania. J Clin Psychiatry. 2010;71(10):1336–1343. PubMed CrossRef
45. Paholpak P, Mendez MF. Trichotillomania as a manifestation of dementia. Case Rep Psychiatry. 2016;2016:9782702. PubMed
46. Crescente Junior JA, Guzman CS, Tavares H. Quetiapine for the treatment of trichotillomania. Rev Bras Psiquiatr. 2008;30(4):402. PubMed CrossRef
47. White MP, Koran LM. Open-label trial of aripiprazole in the treatment of trichotillomania. J Clin Psychopharmacol. 2011;31(4):503–506. PubMed CrossRef
48. Sasaki T, Iyo M. Treatment of puberty trichotillomania with low-dose aripiprazole. Ann Gen Psychiatry. 2015;14(1):18. PubMed CrossRef
49. Virit O, Selek S, Savas HA, et al. Improvement of restless legs syndrome and trichotillomania with aripiprazole. J Clin Pharm Ther. 2009;34(6):723–725. PubMed CrossRef
50. Howard AK, Krishnamoorthy A, Leavitt BR, et al. Treatment of Huntington disease and comorbid trichotillomania with aripiprazole. J Neuropsychiatry Clin Neurosci. 2015;27(3):e211–e212. PubMed CrossRef
51. Sharma V, Baczynski C. Trichotillomania and bipolar disorder. Am J Psychiatry. 2017;174(2):186. PubMed CrossRef
52. Grant JE, Redden SA, Leppink EW, et al. Sex differences in trichotillomania. Ann Clin Psychiatry. 2016;28(2):118–124. PubMed
53. Leombruni P, Gastaldi F. Oxcarbazepine for the treatment of trichotillomania. Clin Neuropharmacol. 2010;33(2):107–108. PubMed CrossRef
54. Lochner C, Seedat S, Niehaus DJ, et al. Topiramate in the treatment of trichotillomania: an open-label pilot study. Int Clin Psychopharmacol. 2006;21(5):255–259. PubMed CrossRef
55. Samuni Y, Goldstein S, Dean OM, et al. The chemistry and biological activities of N-acetylcysteine. Biochim Biophys Acta. 2013;1830(8):4117–4129. PubMed CrossRef
56. Dean O, Giorlando F, Berk M. N-acetylcysteine in psychiatry: current therapeutic evidence and potential mechanisms of action. J Psychiatry Neurosci. 2011;36(2):78–86. PubMed CrossRef
57. Dodd S, Dean O, Copolov DL, et al. N-acetylcysteine for antioxidant therapy: pharmacology and clinical utility. Expert Opin Biol Ther. 2008;8(12):1955–1962. PubMed CrossRef
58. Grados MA, Atkins EB, Kovacikova GI, et al. A selective review of glutamate pharmacological therapy in obsessive-compulsive and related disorders. Psychol Res Behav Manag. 2015;8(8):115–131. PubMed CrossRef
59. Grant JE, Odlaug BL, Kim SW. N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch Gen Psychiatry. 2009;66(7):756–763. PubMed CrossRef
60. Barroso LAL, Sternberg F, Souza MNIFE, et al. Trichotillomania: a good response to treatment with N-acetylcysteine. An Bras Dermatol. 2017;92(4):537–539. PubMed CrossRef
61. Odlaug BL, Grant JE. N-acetyl cysteine in the treatment of grooming disorders. J Clin Psychopharmacol. 2007;27(2):227–229. PubMed CrossRef
62. Rodrigues-Barata AR, Tosti A, Rodríguez-Pichardo A, et al. N-acetylcysteine in the treatment of trichotillomania. Int J Trichology. 2012;4(3):176–178. PubMed CrossRef
63. Özcan D, Seçkin D. N-Acetylcysteine in the treatment of trichotillomania: remarkable results in two patients. J Eur Acad Dermatol Venereol. 2016;30(9):1606–1608. PubMed CrossRef
64. Grant JE, Chamberlain SR, Redden SA, et al. Placebo response in trichotillomania. Int Clin Psychopharmacol. 2017;32(6):350–355. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!


