ABSTRACT
Objective: To evaluate traditional versus guided cognitive-behavioral therapy (CBT) with the use of applications and technological innovations.
Data Sources: A systematic search was conducted in the MEDLINE/PubMed, SciELO, and Cochrane Library databases and included randomized controlled trials (RCTs) from inception to March 30, 2023, with no language restrictions. Only RCTs with available text were included, which is valid from the app versus traditional CBT comparison perspective. The search terms were “apps” OR “app” AND “cognitive behavior therapy” OR “self-guided cognitive behavioral therapy” OR “cognitive behavior therapy” OR “CBT” OR “self-guided CBT” OR “iCBT” OR “unguided iCBT.”
Study Selection: Six RCTs were included in this review.
Results: The results of all the studies were positive for the use of applications and the internet, and the findings were encouraging for new methods of guided therapy and the inclusion of technology.
Conclusions: There is a need for studies that assess the mental health of individuals using and supporting technology, but these findings are encouraging for the continuation of the research.
Prim Care Companion CNS Disord 2024;26(2):23r03566
Author affiliations are listed at the end of this article.
Globally, access to evidence-based psychological treatment is limited. Innovative self-help methods using smartphone applications and low-cost virtual reality have the potential to significantly improve the accessibility and scalability of psychological treatments.
Access to evidence-based psychological treatment for mental health disorders is a global challenge due to high treatment costs and limited availability of mental health professionals. Treatment coverage is below 50% and usually substantially lower. Novel technologies may contribute to accessible and affordable treatment options in important ways.1,2
Such interventions can be administered in either a guided or self-guided fashion. In guided treatments, the patient is supported by a clinician who provides brief support as the individual works through the internet program. Self-guided interventions do not involve clinician support during the intervention. However, it is important to note that there is considerable variability in the delivery of self-guided internet-based cognitive-behavioral therapy (iCBT). For example, some studies have significant involvement with a clinician during the recruitment stage and involve a pretreatment assessment interview via telephone, while others are fully automated with no clinician involvement during any aspect of the study (ie, recruitment, assessment, or treatment). Those that include contact with a clinician at any point of the study may increase supportive accountability,3 which may subsequently lead to enhanced outcomes.4
Some professionals have restrictions with technology and others do not have time to learn, while some use technology as a resource for psychological and therapeutic work, including those who specialize in improving the understanding of the subject.5 Additionally, some people limit themselves from accepting treatments and technological resources due to personal issues or beliefs.
App-based treatments to improve mental health are an increasingly popular method of service delivery, though research on the efficacy of these apps is limited.2,6 Initial evidence of technology-driven delivery of standard treatment protocols for clinical disorders such as CBT for anxiety have demonstrated effect sizes comparable to conventional or traditional standards of care.7
The transition from in-person professional administration of CBT to digital, self-directed delivery was hypothesized to overcome many treatment barriers.8 A recent systematic review and meta-analysis9 of internet- and computer-delivered CBT for youth confirmed the positive effects of these interventions on symptom reduction. However, adherence to many of these interventions is low despite the alignment of digital CBT with young people’s help-seeking preferences.8 This study aimed to evaluate traditional versus guided behavioral therapy with the use of applications and technological innovations.
METHODS
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.10 A systematic search was conducted in the MEDLINE/PubMed, SciELO, and Cochrane Library databases from inception to March 30, 2023, with no language restrictions. Only randomized controlled trials (RCTs) with available text were included, which is valid from the app versus traditional CBT comparison perspective. In this comparison, we included articles that evaluated app versus traditional treatment for anxiety and comorbid disorders. We also included studies that reported on traditional treatments with a waiting list, wherein patients have to wait for the treatment to begin, or other factors that did not affect the methodological format of the research. Duplicates, unavailable studies, and studies with children or the elderly were excluded.
Study Selection
The search terms were “apps” OR “app” AND “cognitive behavior therapy” OR “self-guided cognitive behavioral therapy” OR “cognitive behavior therapy” OR “CBT” OR “self-guided CBT” OR “iCBT” OR “unguided iCBT.”
Eligible studies included RCTs comparing unguided iCBT with guided CBT or against any type of control condition (business as usual, waiting list) in adults with anxiety symptoms, as established by specified cutoff points on self-report scales or diagnostic interviews. Studies were excluded if the intervention did not include cognitive restructuring as a major component, if unguided CBT was combined with traditional treatment, if symptoms other than anxiety were targeted, and if children or the elderly were targeted. Two authors (L.P. and L.A.Q.) selected the studies to be included. Discrepancies were resolved by a third author (A.E.N.).
Data Extraction and Quality Score
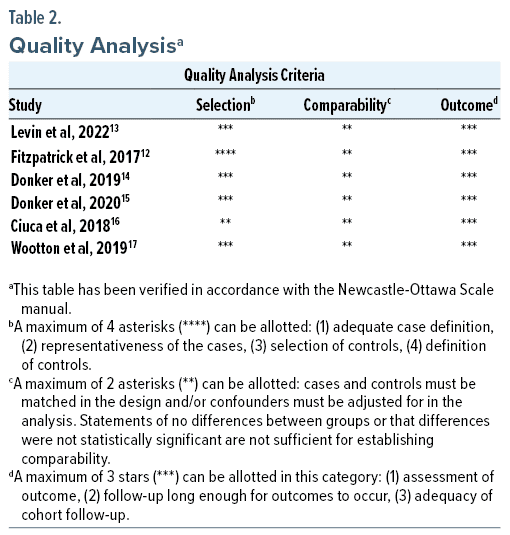
The following variables were extracted from the studies: authors, year of publication, study design, and main outcome. Quality assessment was performed using the Newcastle-Ottawa Scale.11 Data were extracted by 2 authors (L.P. and L.A.Q.), and all authors agreed with the final inclusion of studies in the systematic review, data abstraction, and quality assessment.
RESULTS
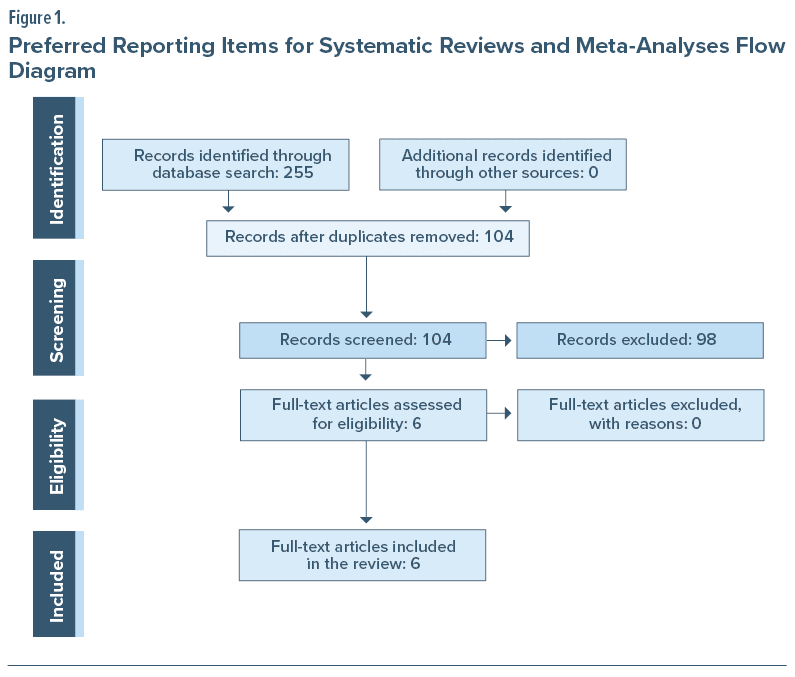
The search yielded a total of 255 studies. No additional studies were identified through a manual search of references. After the elimination of duplicates, 104 articles were screened, and 98 articles were excluded for being outside the proposed theme or subject, leaving 6 selected articles for the final review (Figure 1).
There are some similarities between the 6 articles that describe research findings on anxiety and mental health with the use of internet-enabled applications or devices. Table 1 describes the articles included in the review, and Table 2 provides the quality analysis.
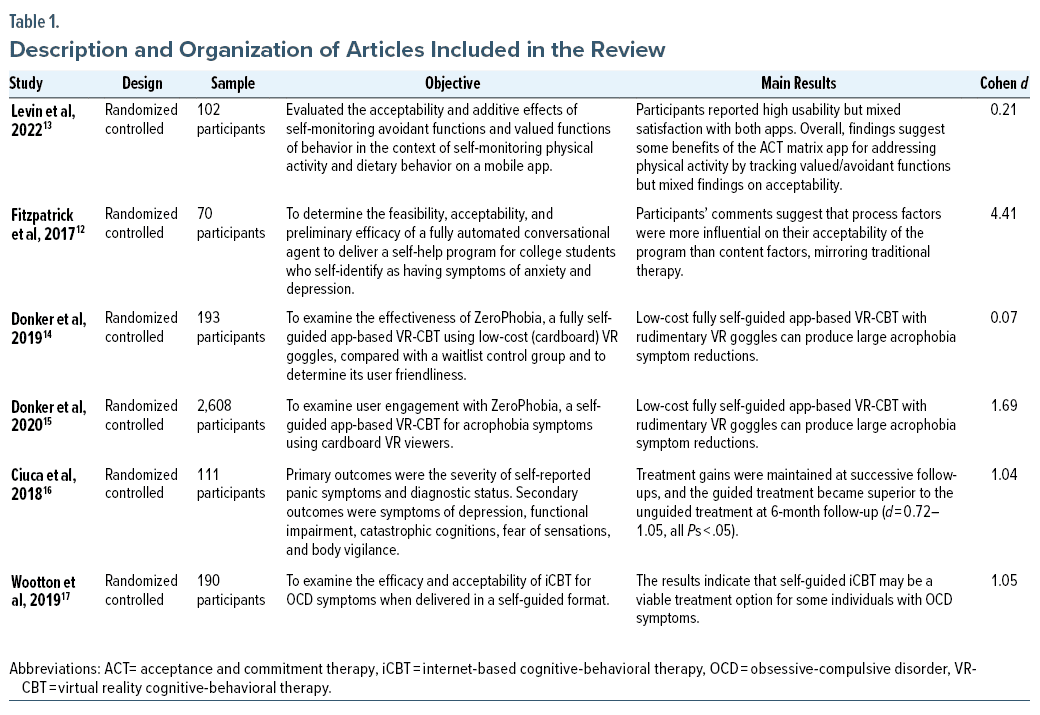
Fitzpatrick et al12 reported that iCBT apps have demonstrated efficacy but are characterized by poor adherence, although conversational agents may offer a convenient, engaging way of getting support at any time. Their study aimed to determine the feasibility, acceptability, and preliminary efficacy of a fully automated conversational agent to deliver a self-help program for college students who self-identify as having symptoms of anxiety and depression. Participants’ comments suggest that process factors were more influential on their acceptability of the program than content factors, mirroring traditional therapy.12
Another controlled trial13 evaluated the acceptability and additive effects of self-monitoring avoidant and randomized valued functions of behavior on a mobile app in the context of self-monitoring physical activity and behavior. The self-monitoring approach was based on the acceptance and commitment therapy (ACT) matrix. A sample of 102 adults interested in improving their diet and physical activity were randomized to a health behavior tracking (HBT) app, HBT plus ACT matrix (HBT + ACT) app, or waitlist condition. Online self-report assessments were completed at baseline, mid-intervention (2 weeks), and post-intervention (4 weeks). Participants reported high usability but mixed satisfaction with both apps.13
Two articles explored the treatment of anxiety with applications for specific phobias using virtual reality. One of the studies14 examined the effectiveness of ZeroPhobia, a fully self-guided, app-based virtual reality (VR) CBT for acrophobia using low-cost (cardboard) VR goggles compared with a waitlist control group to determine its user friendliness. In total, 193 participants were randomly assigned to the intervention (n = 96) or a waitlist control group (n = 97). An intent-to-treat analysis showed a significant reduction of posttest acrophobia symptoms at 3 months for the VR-CBT app compared with the controls. Sensitivity and robustness analysis confirmed the findings. Pretreatment attrition was 22 of 96 (23%) due to smartphone incompatibility. Of the 74 participants who started using the VR-CBT app, 57 (77%) completed the intervention in full.14 The other study15 also looked at app anxiety treatment using virtual reality and included 96 adult participants using ZeroPhobia. Results showed an optimum exposure level at which increasing practice time does not result in increased benefit. Self-guided VR acrophobia treatment is effective and leads to consistent reductions in self-reported anxiety both between levels and after treatment. Most participants progressed effectively to the highest self-exposure level despite the absence of a therapist.15
Another 3-arm RCT16 compared the efficacy of guided with unguided iCBT (12 weeks intervention) and a waitlist. A total of 111 individuals meeting the diagnostic criteria for panic disorder were randomly assigned to 1 of 3 conditions. Primary outcomes were the severity of self-reported panic symptoms and diagnostic status. Secondary outcomes were symptoms of depression, functional impairment, catastrophic cognitions, fear of sensations, and body vigilance. At posttreatment, both active conditions showed superior outcomes regarding panic disorder and associated symptoms. The 2 active conditions did not differ significantly in posttreatment self-reported symptom reduction, but the guided treatment was superior to the unguided treatment in terms of diagnostic status. Treatment gains were maintained at successive follow-ups, and the guided treatment became superior to the unguided treatment at 6-month follow-up.16
The final study17 examined the efficacy and acceptability of iCBT for obsessive-compulsive disorder (OCD) symptoms when delivered in a self-guided format. In this study, 190 participants were randomized to either a self-guided iCBT condition or a waitlist control group. A total of 140 participants completed the baseline assessment, initiated treatment, and were included in the analyses. The between-group effect size at posttreatment was large on the self-reported version of the Yale-Brown Obsessive-Compulsive Scale. Twenty-seven percent of the iCBT condition met conservative criteria for clinically significant change at posttreatment, which increased to 38% at 3-month follow-up. Participants rated the program as highly acceptable. The results indicate that self-guided iCBT may be a viable treatment option for some individuals with OCD symptoms.17
DISCUSSION
Studies show that iCBT packages aiming to be effective and efficient might choose to include beneficial components and exclude those that are potentially detrimental. Web apps can facilitate shared decision-making by the therapist and patient in choosing their preferred iCBT package.12–14,18
Research to synthesize the literature on digital CBT for depression and anxiety in young people has been conducted. These investigations aimed to describe how appropriate use was defined and communicated to users and how adherence was measured, as well as to determine associations between adherence and treatment outcomes.19
Appropriate usage definitions are unique to each digital CBT intervention. However, appropriate usage statements are not systematically reported in the literature. Furthermore, the extent to which usage recommendations are communicated to users is also not regularly reported. Despite appropriate single usage definitions, adherence was generally operationalized generically as the degree of completion of the intervention and was not consistently associated with outcomes. As seen in the RCTs included in this review, preparation and structure are necessary for these new processes using the internet and technology to be considered in an organized way by users.12–15,17 Offering iCBT is an effective and acceptable alternative to therapist-administered treatments for anxiety and depression.12–17,20
Ongoing research shows the aforementioned beneficial effects of iCBT for self-guided patients, but these effects remain incipient. While studies are reportedly planned and in progress, which is encouraging, more work is needed to establish noninferiority to current first-line treatments, explore momentum for change, establish optimal levels of guidance, investigate cost-effectiveness, measure adverse events, and determine predictors of dropout.12,14–17,20
The effects of the treatment on quality of life and the improvements received by the patient with the intervention were also evaluated in some studies, showing the remission of anxiety symptoms in adults.12,14–17,21 Therapist-supported iCBT appears to be an effective treatment for anxiety in adults. Evidence comparing therapist-supported iCBT with waiting list, care, information, or control-only online discussion groups was of low to moderate quality; evidence comparing therapist-supported iCBT with unguided iCBT was of very low quality; and therapist-supported iCBT comparisons with face-to-face CBT were of low quality. Further research is required to better define and measure any potential harm resulting from treatment. These findings suggest that therapist-supported iCBT is more effective than waiting list, care, information, or control-only online discussion groups and that there may not be a significant difference in outcome between unguided CBT and therapist-supported iCBT; however, this latter judgment should be interpreted with caution due to imprecision.21 Evidence suggests that therapist-supported iCBT may not be significantly different from face-to-face CBT in reducing anxiety. Future research should explore heterogeneity among studies that meet the quality of the body of evidence, involve equivalence trials comparing iCBT and face-to-face CBT, examine the importance of the therapist’s role in iCBT, and include iCBT strength trials in real-world settings.18–21
This review shows that there are already positive findings for further research using iCBT with the use of self-guided applications. Of the 6 randomized studies, good results were found in different subtypes of pathology with anxiety, such as OCD, panic disorder, and phobia, with a variety of patients using apps and self-guided therapy. It is clear from the results of the 6 studies that further research is required to validate findings on the use of applications for psychological and clinical treatment.12–17 It should be emphasized that the results were positive for the use of iCBT and encouraging for new methods of guided therapy and the inclusion of technology.
CONCLUSION
This systematic review adds to the development of innovative and scalable delivery methods of evidence-based treatments and underscores that these new technologies have the potential to transform mental health care worldwide.14 To be effective and efficient, iCBT packages may include beneficial components and exclude those that are potentially detrimental. Web apps can facilitate shared decision-making by the therapist and patient in choosing their preferred iCBT package.18
In addition to further studies, it will always be necessary to specify the clinical demand based on the formats that the applications and technologies can offer. The aim should be to provide the best of the available therapies and to expand research to include more patients and providers in a greater variety of treatments.
Article Information
Published Online: March 21, 2024. https://doi.org/10.4088/PCC.23r03566
© 2024 Physicians Postgraduate Press, Inc.
Submitted: May 18, 2023; accepted September 26, 2023.
To Cite: Pelucio L, Quagliato LA, Nardi AE. Therapist-guided versus self-guided cognitive behavior therapy: a systematic review. Prim Care Companion CNS Disord. 2024;26(2):23r03566.
Author Affiliations: Universidade Federal do Rio de Janeiro, Instituto de Psiquiatria, Depression Resistant Ambulatory, Rio de Janeiro RJ, Brazil (all authors).
Corresponding Author: Luísa Pelucio, MD, Rua Norberto Froes de Andrade, 27, apt 102, Santa Rosa, Barra Mansa–RJ 27.323-050 ([email protected]).
Relevant Financial Relationships: Antonio Egidio Nardi is a researcher funded by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (National Council for Scientific and Technological Development) (CNPq) and Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (Carlos Chagas Filho Foundation for Research Support of the State of Rio de Janeiro) (FAPERJ). The other authors declare no conflict of interest.
Funding/Support: None.
ORCID: Luísa Pelucio: https://orcid.org/0000-0002-7928-2578; Laiana A. Quagliato: https://orcid.org/0000-0002-6928-5847; Antonio Egidio Nardi: https://orcid.org/0000-0002-2152-4669
Clinical Points
- Specific strategies and usage definitions are needed to aid physicians in the use of technology-based therapy and improve patient care.
- Barriers to successful technology-based treatment should be addressed if applicable, such as access to the use of apps and the internet and emotional openness to new treatment formats.
- Use of the internet and technology as a support in treatment can be helpful given that many people have access to a smartphone.
References (21)

- Kessler RC, Berglund PA, Bruce ML, et al. The prevalence and correlates of untreated serious mental illness. Health Serv Res. 2001;36(6 Pt 1):987–1007. PubMed
- Fairburn CG, Patel V. The impact of digital technology on psychological treatments and their dissemination. Behav Res Ther. 2017;88:19–25. PubMed CrossRef
- Mohr DC, Cuijpers P, Lehman K. Supportive accountability: a model for providing human support to enhance adherence to eHealth interventions. J Med Internet Res. 2011;13(1):e30. PubMed CrossRef
- Boettcher J, Berger T, Renneberg B. Does a pre-treatment diagnostic interview affect the outcome of internet-based self-help for social anxiety disorder? a randomized controlled trial. Behav Cogn Psychother. 2012;40(5):513–528. PubMed CrossRef
- Bostock S, Crosswell AD, Prather AA, et al. Mindfulness on-the-go: effects of a mindfulness meditation app on work stress and well-being. J Occup Health Psychol. 2019;24(1):127–138. PubMed CrossRef
- Donker T, Petrie K, Proudfoot J, et al. Smartphones for smarter delivery of mental health programs: a systematic review. J Med Internet Res. 2013;15(11):e247. PubMed CrossRef
- Berger T, Boettcher J, Caspar F. Internet-based guided self-help for several anxiety disorders: a randomized controlled trial comparing a tailored with a standardized disorder-specific approach. Psychotherapy (Chic). 2014;51(2):207–219. PubMed CrossRef
- Garrido S, Millington C, Cheers D, et al. What works and what doesn’t work? A systematic review of digital mental health interventions for depression and anxiety in young people. Front Psychiatry. 2019;10(11):759. PubMed CrossRef
- Christ C, Schouten MJ, Blankers M, et al. Internet and computer-based cognitive behavioral therapy for anxiety and depression in adolescents and young adults: systematic review and meta-analysis. J Med Internet Res. 2020;22(9):e17831. PubMed CrossRef
- Page MJ, McKenzie JE, Bossuyt PM, et al. Declaracion PRISMA 2020: Una Guia Actualizada Para La Publicacion De Revisiones Sistematicas. (The PRISMA 2020 statement: an updated guideline for reporting systematic reviews). Rev Esp Cardiol (Engl Ed). 2021;74(9):790–799.
- Gierisch JM, Beadles C, Shapiro A, et al. Health Disparities in Quality Indicators of Healthcare Among Adults with Mental Illness [Internet]. Washington (DC): Department of Veterans Affairs (US); 2014 Oct. Appendix B, Newcastle-Ottawa Scale Manual for Cohort Studies. Accessed February 15, 2024. https://www.ncbi.nlm.nih.gov/books/NBK299087/
- Fitzpatrick KK, Darcy A, Vierhile M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): a randomized controlled trial. JMIR Ment Health. 2017;4(2):e19. PubMed CrossRef
- Levin ME, Krafft J, Seifert S, et al. Tracking valued and avoidant functions with health behaviors: a randomized controlled trial of the acceptance and commitment therapy matrix mobile app. Behav Modif. 2022;46(1):63–89. PubMed CrossRef
- Donker T, Cornelisz I, van Klaveren C, et al. Effectiveness of self-guided app-based virtual reality cognitive behavior therapy for acrophobia: a randomized clinical trial. JAMA Psychiatry. 2019;76(7):682–690. PubMed CrossRef
- Donker T, Klaveren CV, Cornelisz I, et al. Analysis of usage data from a self-guided app-based virtual reality cognitive behavior therapy for acrophobia: a randomized controlled trial. J Clin Med. 2020;9(6):1614. PubMed CrossRef
- Ciuca AM, Berger T, Crişan LG, et al. Internet-based treatment for panic disorder: a three-arm randomized controlled trial comparing guided (via real-time video sessions) with unguided self-help treatment and a waitlist control. PAXPD study results. J Anxiety Disord. 2018;56:43–55. PubMed CrossRef
- Wootton BM, Karin E, Titov N, et al. Self-guided internet-delivered cognitive behavior therapy (ICBT) for obsessive-compulsive symptoms: A randomized controlled trial. J Anxiety Disord. 2019;66:102111. PubMed CrossRef
- Furukawa TA, Suganuma A, Ostinelli EG, et al. Dismantling, optimizing, and personalizing internet cognitive behavioral therapy for depression: a systematic review and component network meta-analysis using individual participant data. Lancet Psychiatry. 2021;8(6):500–511. PubMed CrossRef
- Li SH, Achilles MR, Werner-Seidler A, et al. Appropriate use and operationalization of adherence to digital cognitive behavioral therapy for depression and anxiety in youth: systematic review. JMIR Ment Health. 2022;9(8):e37640. PubMed CrossRef
- Simon N, Robertson L, Lewis C, et al. Internet-based cognitive and behavioral therapies for post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst Rev. 2021;2021(5):CD011710. PubMed CrossRef
- Olthuis JV, Watt MC, Bailey K, et al. Therapist-supported Internet cognitive behavioral therapy for anxiety disorders in adults. Cochrane Database Syst Rev. 2016;3(3):CD011565. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





