
Prim Care Companion CNS Disord 2022;24(6)21cr03229
To cite: Spiegel DR, Parkerson JA, Hammond PB, et al. A case of the Richardson syndrome variant of progressive supranuclear palsy with apathy and depression: clinical evaluation and symptomatic treatment. Prim Care Companion CNS Disord. 2022;24(6):21cr03229.
To share: https://doi.org/10.4088/PCC.21cr03229
© 2022 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
*Corresponding author: David R. Spiegel, MD, Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, 825 Fairfax Ave, Norfolk, VA 23507 ([email protected]).
Progressive supranuclear palsy (PSP), a rare neurodegenerative condition, is the most common cause of atypical parkinsonism. Its most common phenotype, Richardson syndrome (RS), is characterized by prominent postural instability, supranuclear vertical gaze palsy, and cognitive dysfunction.1 Additionally, neuropsychiatric features include apathy and depressive symptoms.2
In the absence of reliably validated biomarkers, the diagnosis is based mainly on clinical criteria. We present the case of a patient who, with lethality, had symptoms of possible/probable PSP-RS. We review the diagnostic process and neuropsychological and neuropsychiatric features of PSP-RS.
Case Report
The patient was a 66-year-old White man who was brought to the hospital after an interrupted suicide attempt. The patient had been admitted to the internal medicine department and started on venlafaxine 37.5 mg/d due to “depression” 3 weeks prior to this admission. The patient reported that his depressed symptoms developed over the past 2 months, coinciding with poor work performance. The patient denied previous psychiatric history, including alcohol and prescription/illicit substance misuse. The mental status examination was remarkable for dysarthria and delayed psychomotor processing speed.
The patient’s medical history was remarkable for an 8-foot fall about 1.5 years ago, without loss of consciousness or further evaluation. About 1 month before that fall, the patient reported difficulties with balance. Subsequently, the patient and his family reported unexplainable falls until this admission.
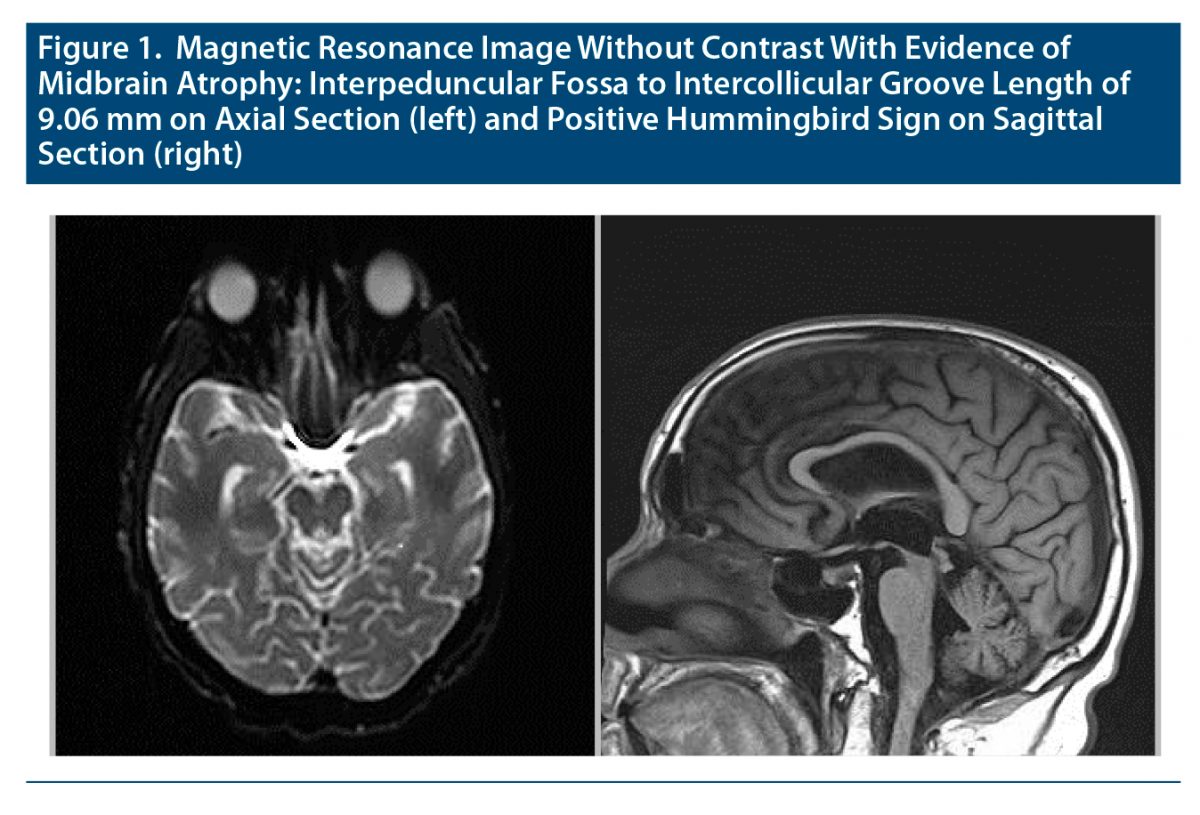
Figure 1 provides the patient’s magnetic resonance imaging results. The patient’s Neuropsychiatric Inventory–Questionnaire (NPI-Q)3 score was 12, with severe and moderate scores on apathy/indifference and depression, respectively. Table 14–6 provides the patient’s physical, neurologic, and cognitive examination results along with the criteria of the National Institute of Neurologic Disorders and Stroke and the Society for PSP (NINDS-SPSP). Due to apathy and depression, venlafaxine was titrated to 150 mg/d. The patient was discharged after a 10-day hospitalization, with an NPI-Q score of 9. At 2-month follow-up, his NPI-Q score decreased to 4, with improvement in both apathy and depression subscales.
While the patient’s diagnosis of probable PSP-RS was based on NINDS-SPSP criteria,5 the latter evaluates 2 core functional domains (ocular motor dysfunction, postural instability). The patient also had impairments in additional domains purported by the Movement Disorder Society–PSP criteria: akinesia and cognitive dysfunction.6
Discussion
The order of appearance of cardinal deficits is highly variable in PSP, although classification in its first 2 years after onset may allow for a more comprehensive description of the PSP phenotypic spectrum.7 For instance, and similar to our patient, the initial symptom in approximately two-thirds of RS patients is postural instability.8 Shortly thereafter, falls develop within the first year of onset. Subsequently, abnormal saccades, bradykinesia, and then vertical supranuclear gaze palsy typically manifest by year 2.7
Alternatively, within 1 year of onset, approximately one-third of RS patients have cognitive changes, summarized as a dysexecutive frontal syndrome.9 Bradyphrenia, a cardinal cognitive feature of PSP-RS, has been shown to progressively deteriorate throughout the course of the illness.10
Apathy and depression, potentially independent constructs, are commonly although not uniformly reported in PSP-RS.11 Disruptions to cortical circuits associated with depression are reported to be far less affected than those associated with apathy.11 Thus, the psychosocial aspects of coping with a chronic/lethal neurodegenerative disease could also explain the pathogenesis of RS patients’ depressive symptoms.
While there is a dearth of evidence for treating apathy or depression in PSP, we continued and increased our patient’s venlafaxine dosage. There is evidence, especially if apathy is prominent as in our patient, that serotonin-norepinephrine reuptake inhibitors such as venlafaxine may be useful.12
In conclusion, presence of early gait dysfunction (described as clumsy and stiff) and postural instability is a key feature of PSP-RS that distinguishes it from other parkinsonian syndromes.13 While there is no known treatment to slow the neurodegenerative process of PSP-RS, quality of life can be improved by evaluating and treating behavioral disorders that commonly occur.
Published online: October 27, 2022.
Relevant financial relationships: Dr Spiegel is in the speakers bureaus for Allergen, Alkermes, Otsuka, and IntraCellular but reports no relevant financial relationships. All other authors report no relevant financial relationships.
Funding/support: None.
Patient consent: Consent was verbally received from the patient to publish the case report, and information has been de-identified to protect anonymity.
References (13)

- Liscic RM, Srulijes K, Gröger A, et al. Differentiation of progressive supranuclear palsy: clinical, imaging and laboratory tools. Acta Neurol Scand. 2013;127(5):362–370. PubMed CrossRef
- Gerstenecker A. The neuropsychology (broadly conceived) of multiple system atrophy, progressive supranuclear palsy, and corticobasal degeneration. Arch Clin Neuropsychol. 2017;32(7):861–875. PubMed CrossRef
- Kaufer DI, Cummings JL, Ketchel P, et al. Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J Neuropsychiatry Clin Neurosci. 2000;12(2):233–239. PubMed CrossRef
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. PubMed CrossRef
- Litvan I, Agid Y, Calne D, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP international workshop. Neurology. 1996;47(1):1–9. PubMed CrossRef
- Höglinger GU, Respondek G, Stamelou M, et al; Movement Disorder Society-endorsed PSP Study Group. Clinical diagnosis of progressive supranuclear palsy: the Movement Disorder Society Criteria. Mov Disord. 2017;32(6):853–864. PubMed CrossRef
- Respondek G, Stamelou M, Kurz C, et al; Movement Disorder Society-endorsed PSP Study Group. The phenotypic spectrum of progressive supranuclear palsy: a retrospective multicenter study of 100 definite cases. Mov Disord. 2014;29(14):1758–1766. PubMed CrossRef
- Golbe LI. Progressive supranuclear palsy. Semin Neurol. 2014;34(2):151–159. PubMed CrossRef
- Rittman T, Coyle-Gilchrist IT, Rowe JB. Managing cognition in progressive supranuclear palsy. Neurodegener Dis Manag. 2016;6(6):499–508. PubMed CrossRef
- Ghosh BC, Carpenter RH, Rowe JB. A longitudinal study of motor, oculomotor and cognitive function in progressive supranuclear palsy. PLoS One. 2013;8(9):e74486. PubMed CrossRef
- Gerstenecker A, Duff K, Mast B, et al; ENGENE-PSP Study Group. Behavioral abnormalities in progressive supranuclear palsy. Psychiatry Res. 2013;210(3):1205–1210. PubMed CrossRef
- VandeVrede L, Ljubenkov PA, Rojas JC, et al. Four-repeat tauopathies: current management and future treatments. Neurotherapeutics. 2020;17(4):1563–1581. PubMed CrossRef
- McFarland NR, Hess CW. Recognizing atypical parkinsonisms: “red flags” and therapeutic approaches. Semin Neurol. 2017;37(2):215–227. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





