See letter by Gorelick and reply letter by Vaseel and Uvais
Cannabis, also commonly known as marijuana or weed, is a psychoactive substance derived from the Cannabis sativa plant. Its use is associated with various physical and psychological effects. The primary psychoactive compound in cannabis is delta-9-tetrahydrocannabinol, which interacts with the brain’s endocannabinoid system, regulating various physiological and cognitive functions.1 While cannabis is known for its euphoric and relaxing effects, it can also induce psychotic effects in susceptible individuals.2
Significant reduction or sudden abstinence from heavy and prolonged cannabis use may precipitate cannabis withdrawal syndrome. Symptoms typically appear within 24 to 72 hours after the last use and can last for about 1 to 2 weeks. Common symptoms of cannabis withdrawal include irritability, anxiety, sympathetic autonomic hyperactivity, stomach pain, tremors, sleep disturbances, fever, chills, reduced appetite, restlessness, and headache.3 In some cases, particularly in individuals with a history of heavy and prolonged use, withdrawal can also trigger psychotic symptoms.
Although cannabis-induced psychosis is commonly encountered in clinical practice and described in the literature, cannabis withdrawal psychosis is rarely reported. Here, we describe a case of cannabis withdrawal psychosis and its management.
Case Report
A 36-year-old married man presented to the psychiatry outpatient department with complaints of suspiciousness, irritability, and reduced sleep for more than 2 months. The symptoms began within 3 days of stopping heavy marijuana use, which had been ongoing for more than 1.5 years. The patient reported smoking approximately 2 g of marijuana per day. He experienced suspiciousness, believing that his colleagues were planning to harm him and unknown individuals were following him wherever he went. There were no symptoms indicative of manic or depressive episodes. The patient had no history of psychiatric illness. He reported no misuse of substances other than nicotine. The patient’s paternal uncle had a history of bipolar affective disorder. There was no history of any comorbid medical illnesses. Physical and basic laboratory examinations were within normal limits. The mental status examination revealed an anxious affect and paranoid delusions. The patient was diagnosed with cannabis withdrawal psychosis. Oral risperidone 1 mg per day was initiated. The patient’s symptoms completely resolved within 2 weeks of starting the medication.
Discussion
Cannabis withdrawal is dependent on the amount of consumption precessation, as well as gender, genetic, and environmental factors. Besides the physical signs, the psychiatric symptoms also have been described in the literature. However, psychiatric manifestations are still an infrequent and misunderstood phenomenon.4–6
We conducted a database analysis of literature published in PubMed using the search keyword cannabis withdrawal AND psychosis. No specific time interval was applied in the literature search; however, the search was limited to only English language publications. We identified 11 cases related to cannabis withdrawal psychosis, the characteristics of which are shown in Table 1. The age range of the patients was 19–47 years, with all being male, except for 1 female case. The time from cessation to the onset of psychosis ranged from 2 to 20 days, with most cases occurring within 1 week of stopping cannabis use.
There was no significant difference regarding the role of past psychosis history, as the results showed that both cases with and without a previous history of psychosis were almost equally likely to present with withdrawal psychosis. Similar to our case, the most common presenting symptoms upon withdrawal were delusions, particularly paranoid delusions, along with disorganized speech and behavior in some cases. Some patients also exhibited hallucinations, suicidal ideation, and affective symptoms.
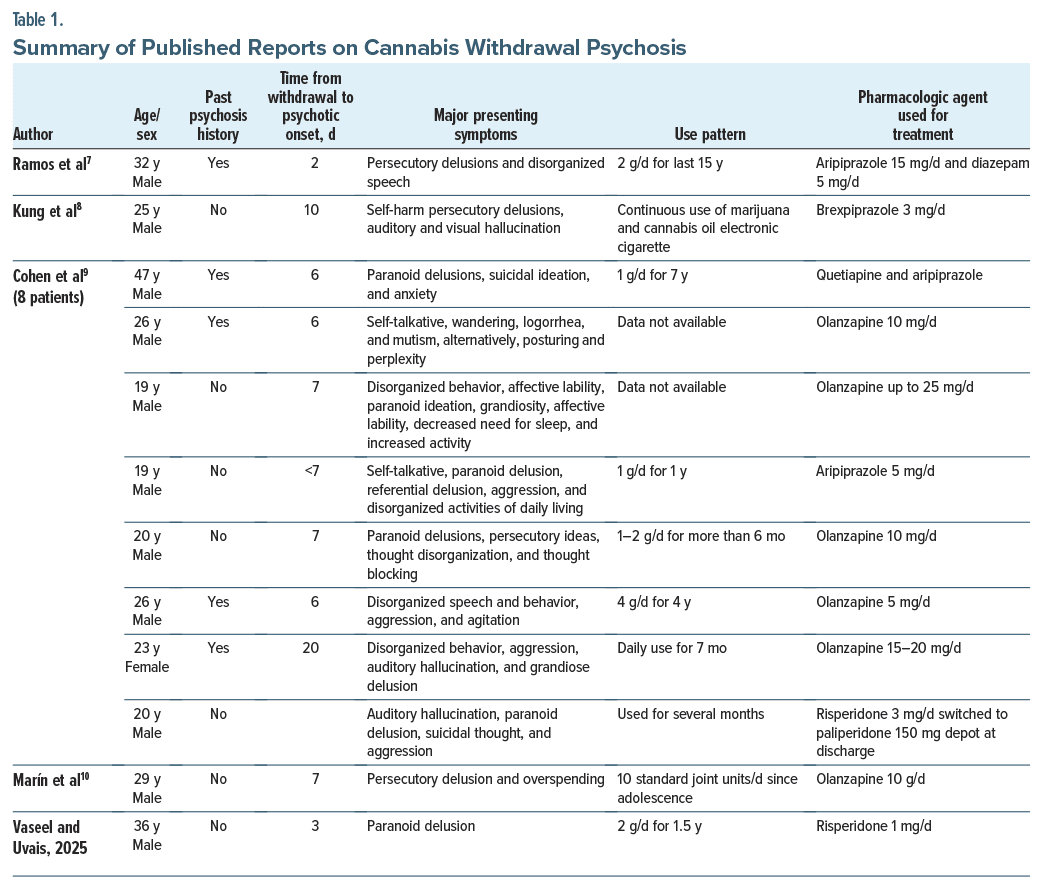
Unlike our case, most of the patients responded to higher doses of second-generation antipsychotic medication. However, our patient became symptom-free with a low dose of risperidone (1 mg for 2 weeks).
Analysis of the characteristics of these cases shows that most instances of cannabis withdrawal psychosis are characterized by heavy and prolonged use of cannabis prior to cessation. Most of the cases with similar presentations were young adults, with onset occurring within 1 week following cessation. We obtained similar results in our case as well. Another important aspect to keep in mind in such clinical scenarios is the potential role of the adulteration of the cannabis in precipitating the psychotic episode.
Article Information
Published Online: January 23, 2025. https://doi.org/10.4088/PCC.24cr03802
© 2025 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2025;27(1):24cr03802
Submitted: June 30, 2024; accepted October 1, 2024.
To Cite: Uvais NA, Vaseel M. Persistent psychosis induced by cannabis withdrawal. Prim Care Companion CNS Disord. 2025;27(1):24cr03802.
Author Affiliations: Department of Psychiatry, Iqraa International Hospital and Research Centre, Calicut, Kerala, India (all authors).
Corresponding Author: N. A. Uvais, MBBS, DPM, Iqraa International Hospital and Research Centre, Malaparamba, Calicut, Kerala 673009, India ([email protected]).
Relevant Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and all information has been de-identified to protect anonymity.
References (10)

- Atakan Z. Cannabis, a complex plant: different compounds and different effects on individuals. Ther Adv Psychopharmacol. 2012;2(6):241–254. PubMed CrossRef
- Johns A. Psychiatric effects of cannabis. Br J Psychiatry. 2001;178(2):116–122. CrossRef
- Connor JP, Stjepanović D, Budney AJ, et al. Clinical management of cannabis withdrawal. Addiction. 2022;117(7):2075–2095. PubMed CrossRef
- Bonnet U, Preuss UW. The cannabis withdrawal syndrome: current insights. Subst Abuse Rehabil. 2017;8:9–37. PubMed CrossRef
- Copersino ML, Boyd SJ, Tashkin DP, et al. Cannabis withdrawal among non-treatment seeking adult cannabis users. Am J Addict. 2006;15(1):8–14. PubMed CrossRef
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
- Ramos B, Santos Martins AF, Lima Osório ES. Psychotic cannabis withdrawal: a clinical case. Cureus. 2022;14(11):e31465. PubMed CrossRef
- Kung FH, Lin HY, Tai YM, et al. Brexpiprazole in the treatment of cannabis withdrawal psychotic disorder. Am J Ther. 2022;29(4):492–493. PubMed CrossRef
- Cohen J, Petitjean H, Blasco MB, et al. Cannabis induced psychotic disorder with onset during withdrawal: a brief report of emerging evidence. Acta Neuropsychiatr. 2024;36(5):325–329. PubMed CrossRef
- Marín J, Pérez de Mendiola X, Fernández S, et al. Cannabis withdrawal induced brief psychotic disorder: a case study during the national lockdown secondary to the COVID-19 pandemic. J Addict Dis. 2021;39(4):579–584. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





